
What did the research involve?
We know that during the pandemic more people than usual died at home. But we don't know as much about the health services those people used and whether the care they received was good quality.
So we used data to look at the end-of-life care people received: for instance, if they went to their GP or had to go to hospital. This information was accessed electronically via the OpenSAFELYplatform. OpenSAFELY is very secure as researchers do not have access to any personal data such as people’s names or addresses.
We also spoke to patients and families with recent experience of end-of-life care to understand their perspectives on the research, and highlight issues of most concern to them.
What were the key findings?
Here's what we found...
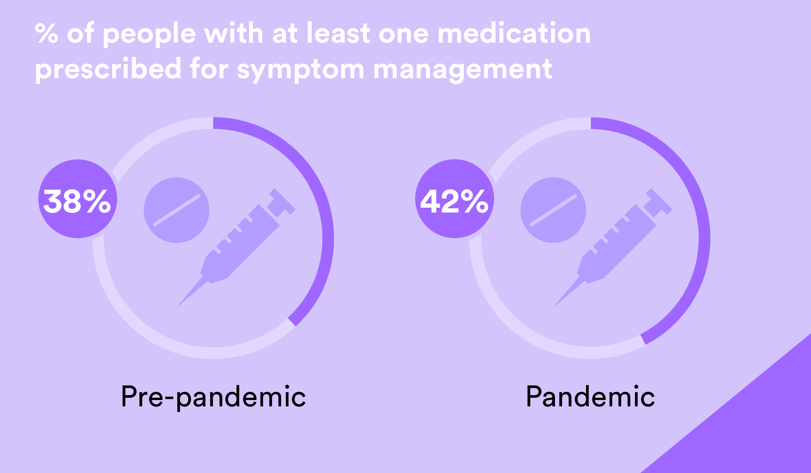
Issues relating to medication near the end of life were seen as the biggest roadblock to a good death.
More medications were prescribed in the pandemic, but patients and their families had poor experiences accessing and using medication towards the end of life, both before and during the pandemic.
For carers, pain relief was a big part of minimising their loved one’s distress.
Patients and their families faced difficulties getting the medication they needed.
- Getting hold of someone to prescribe medication was sometimes difficult, and there was a lack of support in using medication at times.
- People did not always understand exactly what the medication was for, and how and when it should be used. They wanted more information.
- Sometimes syringe drivers were only be offered very close to death. They didn’t always work properly and people weren’t always supported to use them.
- Care was sometimes not very joined-up. For example, sometimes people were sent home from hospital without the medication they needed.
The quality of contact with health services is more important than the quantity.
In the pandemic people actually generally received more support from general practice teams – but this does not necessarily mean they received the care they needed.
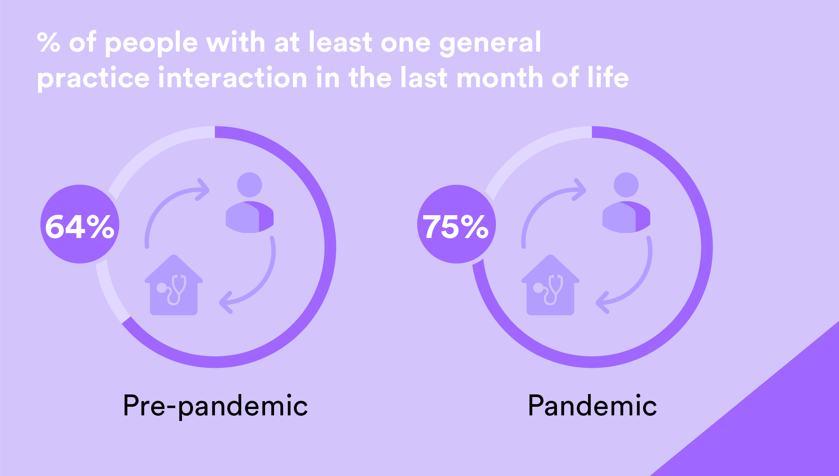
More interactions were remote (e.g. via the telephone), and sometimes it was hard to get through to someone to speak to.
The focus needs to be on whether people’s issues were resolved following their discussions with a professional and whether they got the help they needed.
Some people had concerns that the quality of care was not as good when it was not delivered in person.
For people with Alzheimer's and dementia, informal carers play a particularly vital role.
Patients with dementia or Alzheimer’s who died had more visits to urgent care during the pandemic. This might be because they were struggling to get support at home.
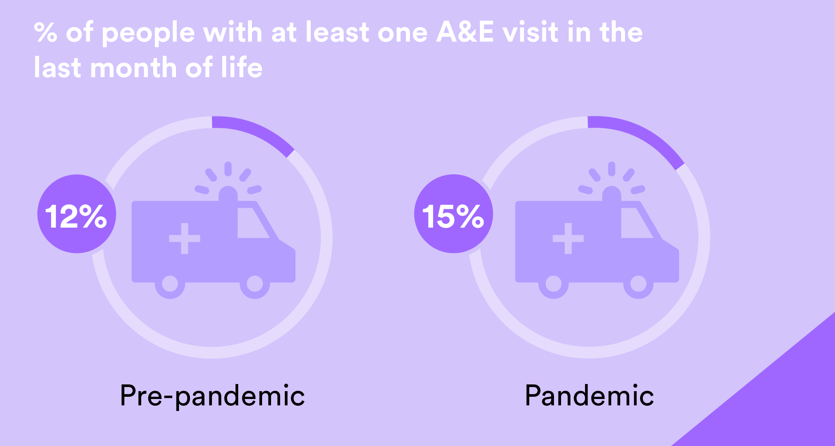
People with Alzheimer's and dementia received less 'informal' care from friends or family during the pandemic. The loss of this care and support may have led to A&E visits and increased GP interactions.
Being in less frequent contact with family during the pandemic may have led to people's health deteriorating without having someone there consistently to advocate, meaning urgent care was needed.
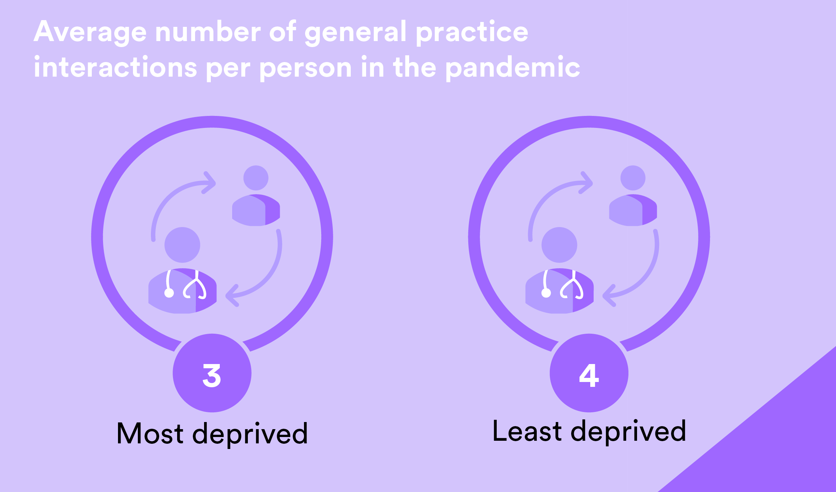
People living in the most deprived areas received fewer services during the pandemic than those in the least deprived areas.
Why might this be? People felt that ‘dying well’ requires people to have a lot of time and energy to pursue their care. There was a feeling that it was necessary to be articulate and persistent, and to have a self-belief that they deserve care.
People highlighted that there is a certain amount of luck involved in dying well. Having access to an excellent GP or a supportive hospice nurse can make all the difference.
So, what needs to happen now?
Integrated care boards are responsible for putting plans in place to meet the health care needs of the local population. They have a legal duty to ensure that palliative care is provided in the local area. Better use of data at a local level would help to identify where any problems with end-of-life care lie, and whether there are specific groups or areas receiving poor care.