

The NHS is not in a position to lose staff. Government commitments to deliver 50,000 more nurses, not to mention thousands more GPs, mental health professionals and physiotherapists, are dependent on improvements in staff retention. The vision for recovering elective services and bringing down unacceptably long waiting times for vital treatments depends on those same people.
But many NHS staff have faced almost unimaginable difficulties during the pandemic, and many studies have reported increased rates of depression, anxiety and severe stress, alongside a range of other serious issues. All the evidence suggests this is leading to more staff choosing to leave the health service.
The pragmatic case for taking the health of staff seriously is indisputable – as is the moral case that an organisation that is all about caring for patients should also care for its staff.
So, how worried should we be about NHS staff health and wellbeing, and what can be done to address serious concerns? We discussed with experts within the health service, as well as researchers who have been trying to understand the problems and provide suitable and effective responses. Some of this is already well understood, and the actions required have also been mapped out based on the evidence. However, our conversations have also uncovered aspects of the issue that have received less attention.
What is the extent of the problem?
There are many worrying anecdotal reports of the dire impact that the pandemic has had on staff, but there exists little systematic data on the issue.
A large-scale survey of the impact of the pandemic on the short and long-term health and wellbeing of all staff found high rates of probable post-traumatic stress disorder (PTSD) (36%), probable common mental disorders (51%) and alcohol misuse (18%). More detailed analysis revealed actual rates of PTSD of around 9%, which is double that in the general population. Women, younger staff and nurses “tended to have poorer outcomes than other staff, except for alcohol misuse”. Staff reporting greater exposure to moral injury (distress resulting from violation of one’s moral code) was strongly associated with increased levels of these problems.1
The only longitudinal analysis of 2,773 workers right across the NHS from more than a quarter of UK trusts (conducted shortly after the first Covid-19 peak in April and May 2020) found that over 21% of health and care workers reported high levels of depression, compared with 5% before the pandemic.
Earlier Nuffield Trust work has described how burnout, job satisfaction and physical working conditions are all key factors contributing to increased GP turnover over the past decade. When surveyed, nurses leaving the register in the year to June 2020 most commonly cited retirement, personal circumstances and too much pressure as their reasons.
The NHS staff survey provides further evidence of a worrying longer-term trend in staff wellbeing and positivity.
Nuffield Trust analysis of NHS staff survey data collected after the first wave of the pandemic in this country found that half (50%) of all staff working with Covid-19 patients experienced illness as a result of work-related stress, compared to 41% of those not working in Covid-19 settings. Fewer staff working in Covid-19 environments felt their organisation took positive action on health and wellbeing (29%, compared with 36% of staff working elsewhere).
And although a much higher proportion of staff working in Covid-19 settings reported working additional paid hours (49% versus 25%), there was no difference between groups in the proportion of staff who worked additional unpaid hours.
A higher proportion of staff working in Covid-19 settings also reported going into work despite not feeling well enough to do so. Nearly a quarter (24%) of these staff reported feeling pressured by colleagues to attend work, which was only true for a fifth of staff not working in Covid-19 settings.
It was not only staff working in high-intensity areas, such as intensive care units, emergency departments and Covid wards who reported a significant negative impact. Community staff reported experiencing increased feelings of isolation, describing their difficulties with using personal protective equipment in home environments and dealing with much higher levels of death among their patients on a daily basis.
Clinically vulnerable staff who were required to shield also experienced problems of isolation, with the additional technological challenges of remote working during a time of crisis. Some had strong feelings of guilt that they were not able to support their colleagues in the way they would have wished.
Senior staff suffered too. Forthcoming Nuffield Trust research finds a less discussed, but significant impact on people in managerial positions, particularly clinical managers. Like many staff, they were working very long hours and many of the decisions they were asked to take were burdensome and difficult to make remotely. Some of these decisions also carried the risk of moral injury. The nature of some of their work also pulled them away from clinical areas to solve problems, which created tensions whereby staff felt their managers had become "invisible", compounding distress on both sides.
In this respect, the use of the term ‘front line’ draws an unhelpful distinction when examining issues of distress, burnout and stress during a crisis.
What needs to be done?
Several common themes arose from the discussions we had with health and wellbeing leads in five NHS trusts. Some of these centre around ensuring the essentials of staff care are in place – others respond more directly to concerns over stress and anxiety.
Improve staff experience
The pandemic has refocused attention on the need to deliver the basics of positive staff experience. These ‘hygiene’ factors were an issue before the pandemic and have, in retrospect, clearly not received sufficient attention.2 While not a solution to more serious issues around wellbeing, staff experience could generally be improved where trusts are able to ensure the following basic provision:
- Staff rooms and rest areas
- Changing facilities
- Hot food at night and at weekends
- Car parking
- Security for staff at night.
In addition, trust rota planning, training and support must ensure that:
- Staff are properly prepared for their roles – they understand what is required and where appropriate are psychologically prepared
- Shift patterns are well designed and flexible to suit the needs of staff as well as the organisation3
- Basic equipment and training programmes are in place
- There are sufficient staff to ensure that care is safe and breaks can be taken
- Appropriate IT and network equipment is provided to promote home working.
Our discussions showed that national initiatives, helplines and support systems seem to have been less valued, and wellbeing leads placed more emphasis on local schemes and peer support.
Create options for dealing with stress
The Trauma Response Group has developed a helpful review of structural approaches to specifically deal with stress and the prevention and management of trauma. Greenberg and colleagues suggest:
- Flexible and responsive deployment of staff – rotating staff between high and lower stress settings, buddying less experienced staff with more experienced colleagues, identifying vulnerable staff and providing proactive support.
- Creating a team spirit and fostering cohesive leadership styles that model a caring approach, encourage formal and informal peer support, and provide space and time for regular opportunities to talk about experiences.
- Providing high quality psychological and wellbeing services that are evidence based, provided by trained staff if interventions are provided and appropriately supervised.
- Communication and feedback mechanisms.
Greenberg and colleagues suggest using an approach based on the principles of proximity, immediacy, expectancy and simplicity. They believe that this “‘de-medicalises’ normal (even uncomfortable) responses and reinforces practical measures that can often be implemented by supervisors”. While it is important to recognise that people are resilient and will often cope, they recommend a relatively low threshold for referral to wellbeing services.
They also identify approaches that may look attractive, but may be ineffective or harmful:
- Generic training, such as mental strength training
- Single interventions that require staff to talk about their thoughts and feelings (this can increase the risks of PTSD)
- Being too quick to use psychological interventions (this may interfere with normal coping mechanisms)
- Psychological debriefing techniques (evidence suggests these are unhelpful and may even cause harm)
- While many ‘wellness’ approaches are popular, such as mindfulness or virtual yoga – and unlikely to cause harm – the evidence of benefit is often limited.
While many of these measures are targeted at individuals, attention to whole teams should also be an important part of the set of actions organisations use.
Two other important, though less obvious, areas of importance for tackling staff stress and burnout emerged from studies and interviews.
Middle management and supervision
The importance of the immediate management and supervisory layer in organisations is generally underappreciated. This group have had particular importance during the pandemic in helping staff to cope and recover.
The style of leadership of this group is vital, as is the ability to support staff and be flexible where necessary (in areas such as rostering and allowing time off) and having the skills to monitor the stress and mental health of staff – and to intervene where necessary. Michael West discusses these aspects and also highlights:
Eight key workplace factors that impact on the wellbeing, flourishing and work engagement of health and social care staff
Chart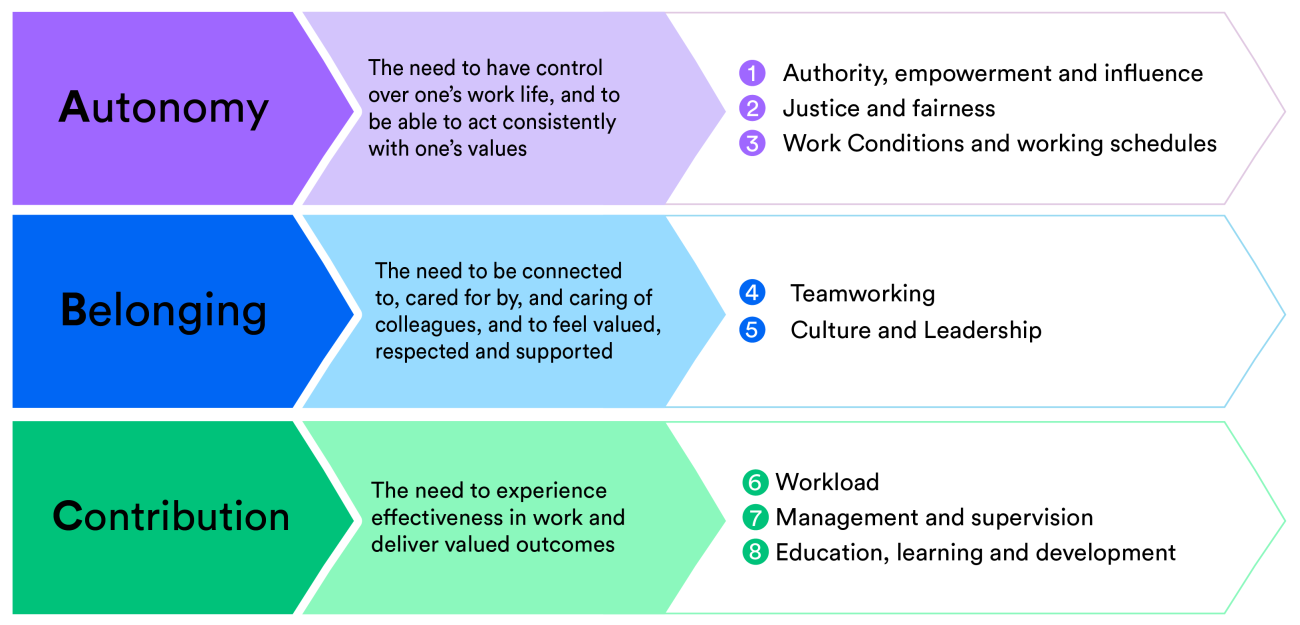
These managers have an important role in connecting staff to the leadership of the organisation, making sense of what is happening or has happened, and helping to create a sense of purpose. Ensuring that the basics required to do the job are in place, innovating to solve problems and removing any obstacles are even more important during a crisis than they are normally.
Measurement, monitoring and communications
Absenteeism and turnover of staff can be measured, but the problem of ‘presenteeism’ (coming to work regardless of illness or stress and then performing sub-optimally) is harder to spot and may even be a bigger problem in terms of lost productivity and the impact on the individual, patients and their colleagues4. More sophisticated measures of employee sentiment are therefore required.
NICE recommends “watchful waiting” for people exposed to situations that carry a risk of PTSD. In addition to systems for monitoring individuals, organisations have also been developing mechanisms for measuring overall staff sentiment, motivation and feedback.
A striking example is Northumbria Healthcare NHS Foundation Trust, which has a comprehensive approach to measuring organisational climate and staff views, with very high response rates thanks to the use of a digital platform, the ability to process free text, and data collected on motivation on a weekly basis. This allows effective and targeted communication to take place, and the different interventions to be monitored close to real-time, with adjustments and actions taken more rapidly.
Conclusions
As in other contexts, Covid-19 has shone a spotlight on concerns that were already recognised. Stress and burnout have always been a problem for medical and nursing staff. Covid-19 has intensified a series of pre-existing problems, while also creating new ones. In doing so, it has highlighted the importance of practices and approaches that staff require for their health and wellbeing regardless of whether or not there is a pandemic.
Some concerns may appear obvious. For example, at what point did the NHS collectively decide that not providing proper staff facilities, hot food at night and other basic amenities was appropriate?
Others are rather more complex organisational and process-based issues that trusts must disentangle. Successful organisations pay attention to the basics of staff experience, the development and support of middle management and supervisors (including giving them the tools to operate in this key role), high quality internal communications, well-designed programmes and rapid and repeated measurement.
There are very few breakthrough innovations. The special ingredient is excellent and continuous delivery.
This work is supported by Allocate Software.