
It is a year since the Government published the outcome of the Spending Review and so fixed public spending allocations for the four years from 2011/12 to 2014/15. The Spending Review led to an 11% reduction in departmental allocations across government (IFS summary of Spending Review, Oct 2010). Health received a comparatively generous allocation with a small real terms increase (0.4% over the four years).
A year on we have additional data from the Treasury and the Department of Health. The Department has also published primary care trust (PCT) allocations and the NHS Operating Plan so the implications of the Spending Review are becoming clearer.
There has been a rumbling debate about how real the real-terms increase in spending for the NHS is. Looking at total departmental planned spending (Departmental Expenditure Limits, or DELs in the jargon), as the chart below shows, two things have been working in opposite directions.
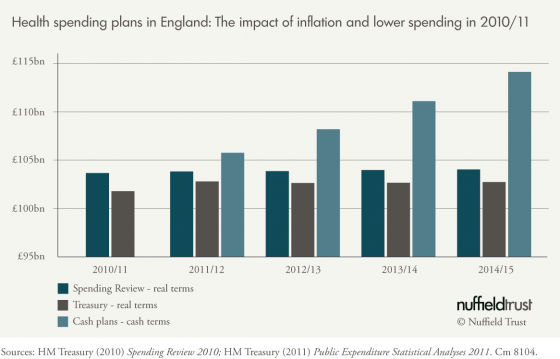
On the one hand, whole-economy inflation is now forecast to be higher: 2.9% in 2011/12 rather than the 1.9% projected at the Spending Review, which means less can be bought by the NHS for any given budget. On the other, the NHS managed to spend less in 2010/11 than its allocation – £1.9 billion lower on a total £101.9 billion budget. Capital spending alone was almost £900 million lower.
However, one thing remains clear: the next four years will be the most challenging in the health service’s history. As the PCT allocations have flowed into contract and commissioning rounds, organisations across the service are coming to grips with this reality.
Recurrent PCT allocations in 2011/12 are increasing by 2.2% (in cash terms) compared to last year’s allocations. This is less than the forecast for whole-economy inflation. In most parts of the country last year’s under-spend suggests PCTs should be able to manage within the tighter funding envelope, especially as pay pressures are mitigated by the impact of the pay freeze for public sector workers earning over £21,500 a year and as management costs fall.
Strategic health authorities (SHAs) and PCTs were forecasting a surplus for 2011/12 of £1,165 million at quarter one. But this picture is not universal: as David Flory’s report on financial quarter one showed, three PCTs in North London are projecting a combined deficit of £56 million this year.
Work by the Audit Commission suggests that there will be further challenges ahead, as almost a quarter of cost improvement plans last year came from one-off savings.
But if 2011/12 is challenging for PCTs it is even more challenging for providers. Two per cent of PCT allocations will be held back by SHAs for one-off projects and, furthermore, SHAs and PCTs have agreed target under-spends. While this may be prudential financial planning for the health system as a whole it puts further pressure on NHS providers, who now need to deliver cost improvement plans of almost 5% this year.
The NHS will only be able to manage against a background of rising demand and an aging population if there is sustained improvement in productivity.
Out of a total target of £5.9 billion PCT QIPP savings for 2011/12, PCTs are seeking £3.1 billion of savings from acute services. As with PCTs overall, across the health service this is likely to be delivered but there are a number of providers whose cost improvement targets are much greater and are projecting deficits – a number of these are also in London. The London trust sector is forecasting a deficit of £107 million at quarter one.
Beyond this year, the outlook is much less certain. The £20 billion efficiency challenge cannot be met by reductions in management costs and the impact of the two-year pay freeze – although they make an important contribution.
The NHS will only be able to manage against a background of rising demand and an aging population if there is sustained improvement in productivity. This means bearing down on unit costs, particularly in the acute sector where spending once again grew faster than activity in 2010/11 (Audit Commission report on annual accounts for NHS for 2010/11).
It also means a step change is needed in providing more effective and efficient pathways of care, particularly for people with chronic disease, to avoid the need for costly hospital treatment. The will and the rhetoric are there: witness the new language in the Health and Social Care Bill on developing integrated care.
But progress is sluggish – for example 2010/11 saw a further small increase in the share of spending in acute hospitals and a reduction in the share of spending in primary care. This issue should demand at least as much management time as managing cutbacks, and progress will not be possible without serious co-production by front-line staff and patients.
This article has also been published on the Guardian Professional website.
Anita appeared on the Today programme on Friday, 7 October to discuss what is happening to NHS finances in England and whether the Government is delivering its pledge to increase health care spending in real terms. Listen to the interview on the BBC website.
Suggested citation
Charlesworth A (2011) ‘What is happening to health spending in England?’. Nuffield Trust comment, 7 October 2011. https://www.nuffieldtrust.org.uk/news-item/what-is-happening-to-health-spending-in-england