
Today marks the launch of primary care co-commissioning between NHS England and the majority of CCGs. These plans support the current direction of travel that aims to see more care being provided in the community as well as services and (perhaps) commissioners integrated. However, for the CCG leaders trying to turn these policy intentions into reality, the pressures facing both commissioners and general practice providers suggest that life is going to get harder before it gets easier.
What does this mean for how likely it is that co-commissioning will deliver on its promises?
The new primary care co-commissioning arrangements between NHS England and CCGs aim to improve health outcomes, reduce inequalities, improve patient experience, improve access to primary care, and make more services available closer to home, amongst others. The policy offers three levels of additional responsibility, and was a voluntary opt-in for CCGs (although how much choice CCG leaders felt they actually had is the subject of another blog).
70 per cent of CCGs have been accepted for delegated or joint arrangements, allowing them varying levels of control over the primary care budget. The remaining CCGs will have greater involvement in NHS England’s decision-making over primary care commissioning in their respective areas.
New research being published today in collaboration with The King’s Fund suggests that CCGs are likely to face a number of challenges in making the new policy work.
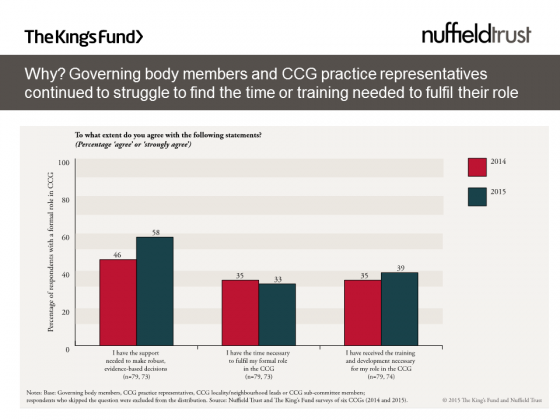
Clinical leaders in the six CCGs that took part in our survey told us that they lacked the time or training necessary to fulfil their existing roles, even before co-commissioning kicks in. This won’t be helped by a 10 per cent reduction in CCGs’ annual running costs that also comes into effect today. The extra capacity that NHS England has proposed to give CCGs to deal with the additional workload of commissioning primary care seems unlikely to provide the support needed and there is competition for the involvement of GP leaders from the growing number of GP-led provider organisations.
A big selling point for primary care co-commissioning is that it builds upon the existing peer-to-peer, supportive relationships that CCG leaders should have developed with their members. However, for those CCGs that will begin to manage practice contracts, our research highlighted the need for careful negotiation when implementing these additional responsibilities.
We found that few GPs felt it was appropriate for their CCGs to use performance management mechanisms, such as setting targets or sanctions for underperformance, to influence their work (as Laura Bennett discusses in her blog). CCGs will need to work hard to ensure that co-commissioning strengthens their relationship with their GP members rather than creating distance, preventing the ‘us and them’ culture for which Primary Care Trusts (PCTs) were often criticised.
A broader question about the future role and function of commissioners is emerging: is commissioning able to achieve what has been asked of it, both in terms of adequately holding local providers to account and achieving marked improvements to patient outcomes? Research into the success of previous incarnations of commissioning has been equivocal in their conclusions (including GP Fundholding, Total Purchasing Pilots, PCTs and Practice-based commissioning).
Or does control over these outcomes lie elsewhere in the system? The large provider organisations being developed as a result of the Five Year Forward View seem set to test this further. Will commissioners be redundant in a large, vertically integrated network?
Co-commissioning has the potential to provide CCGs with the additional levers they need to drive change in primary care and hopefully achieve some of the ambitions set out by NHS England. However, it is not clear how commissioners fit into the vision for new models of care. Increasing the pressure on GP leaders whilst also changing the dynamic between leaders and members could come at the price of clinical engagement in commissioning.