This interactive timeline brings 70 years of reform and change in the National Health Service to life, charting the evolution of this public institution from its inception in the post-war years through to the present day. Scroll down to view the entries chronologically, or use the menu on the left-hand side to jump to a specific decade.
You can also put your knowledge to the test in our fun quiz.
“Medical treatment covering all requirements will be provided for all citizens by a national health service.”
Sir William Beveridge: Social Insurance and Allied Services (The Beveridge Report)
December 1942
Sir William Beveridge’s report, Social Insurance and Allied Services, proposes major changes to create the foundations for a welfare system and, in its support, a national health service (the details are left for later).
Pressure for the creation of a national health service had been building for decades with support from all parties. At the outbreak of the Second World War on 3 September 1939, an Emergency Hospital Service was created and this provided solid foundations for assimilating hospitals into what became the NHS.
The right to medical treatment for everyone under a new national health service is proposed by an inter-departmental committee led by Sir William Beveridge. The committee was asked to: “undertake, with special reference to the inter-relation of the schemes, a survey of the existing national schemes of social insurance and allied services”.
One of the provisions of Beveridge’s committee was that: “medical treatment covering all requirements will be provided for all citizens by a national health service organised under the health departments and post-medical rehabilitation treatment will be provided for all persons capable of profiting by it”.
February 1944
The White Paper, A National Health Service, is published, which was prepared by the Conservative Minister for Health, Henry Willink.
Wide-ranging discussions with the medical professions and health organisations culminate in a complex plan, with cross party support, in which local authorities play a major role.
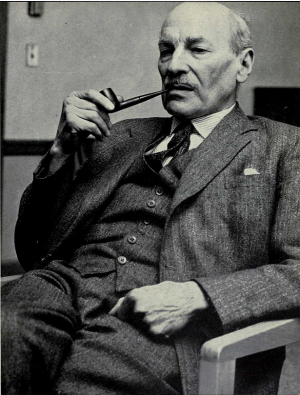
The 1945 British General Election takes place in early July following a month-long campaign.
Both the Conservative and Labour parties commit themselves to ensuring free access to health care services in their respective manifestos. Choice of general practitioner (GP) features prominently as a priority, as does the need to improve maternity services.
Image: Clement Atlee who served as British Prime Minister from 1945 to 1951.
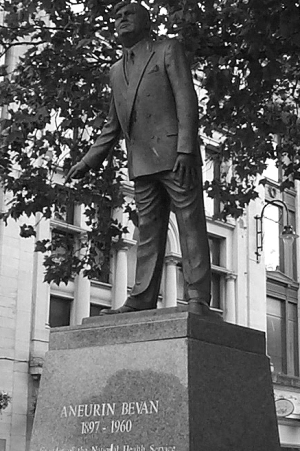
Bevan discards previous compromises and takes new proposals to Cabinet. The proposals include a system based on regions and taking all hospitals into public ownership.
The Act sets out a duty for the Minister of Health to: “promote the establishment in England and Wales of a comprehensive health service designed to secure improvement in the physical and mental health of the people of England and Wales and the prevention, diagnosis and treatment of illness, and for that purpose to provide or secure the effective provision of services... The services provided shall be free of charge, except where any provision of this Act expressly provides for the making and recovery of charges.”
Two years of acrimonious debate follows, with the majority of doctors opposed to the introduction of the National Health Service (NHS). Nye Bevan proves a formidable negotiator and succeeds in overcoming the opposition both of those in his own party who wanted Local Authorities to take a greater part, and the professions who were afraid of losing their independence by becoming state servants on low pay.
“The essence of a satisfactory health service is that the rich and the poor are treated alike, that poverty is not a disability, and wealth is not advantaged.”
Aneurin Bevan, In Place of Fear, Simon and Schuster 1952
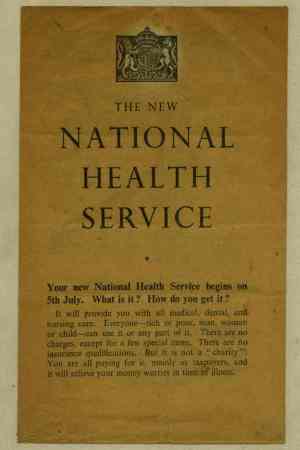
July 1948
The National Health Service (NHS) is created.
The NHS is founded on 5 July 1948, following an official unveiling at Park Hospital (now Trafford General Hospital) in Manchester. 1,143 voluntary hospitals with some 90,000 beds and 1,545 municipal hospitals with 390,000 beds are subsumed within the new NHS.
General practitioners remain self-employed and largely independent, having argued successfully for a contract for service rather than a contract of service.
A new three-part bureaucracy is created to manage the service, comprising: 14 regional hospital boards (RHBs), 36 boards of governors for teaching hospitals (BGs) and 388 hospital management committees (HMCs); 138 executive councils (ECs); and 147 local health authorities (LHAs).
“It is the policy of the Government to relieve nurses of all work not requiring nursing skill.”
Baron Shepherd, House of Lords Chief Whip, House of Lords Debate, 3 May 1949, vol 162, cols 159–98.
May 1949
The Nurses Act 1949 establishes a modern framework for the role of nursing within the NHS. Rising costs give cause for concern.
A depleted labour market after the war means that the Government has begun to look overseas to help increase nursing numbers and the UK sees a large influx of nurses from the Caribbean.
The Nurses Act 1949 enacts many recommendations from the 1946 Wood Committee, which was set up by the Ministry of Health to examine the role of nursing in the new NHS.
The educational role of the [then] nurse regulator – the General Nursing Council (GNC) – is strengthened and a new syllabus for general training is completed and approved in 1952.
December 1949
The NHS is given the power to levy a charge for prescriptions.
The National Health Service Act 1946, which set up the NHS, contains a provision that NHS services should be provided free of charge unless that Act expressly provided for a charge.
Legislation providing for a prescriptions charge is passed by the Labour Government through the NHS (Amendment) Act 1949. This allows for such a charge, and exemptions to it, to be introduced by regulations.
Although the power is introduced in 1949, the charge itself is not introduced until 1952.
“The overall state of general practice [in England] is bad and still deteriorating.”
Collings JS (1950), ‘General practice in England today: a reconnaissance’ The Lancet i, 555–85.
March 1950
JS Collings’ survey of English general practice, funded by the Nuffield Trust, is published in The Lancet.
JS Collings, an Australian research fellow at the Harvard University School of Public Health, is commissioned by the Nuffield Trust to undertake a survey of general practice in England.
His report, published in The Lancet, is damning. He finds that: “the overall state of general practice is bad and still deteriorating”; “some [working conditions] are bad enough to require condemnation in the public interest”; and inner-city practice is “at best... very unsatisfactory and at worst a positive source of public danger”.
His report is followed by further studies; leading ultimately to the foundation of the College of General Practitioners in 1952; and slowly, more government action to assist the development of general practice.
3.5% UK spending on the NHS as a share of GDP
April 1951
The new Chancellor of the Exchequer, Hugh Gaitskell, proposes a one shilling (5p) prescription charge and new charges for dental treatments (chiefly dentures) and spectacles.
Aneurin Bevan resigns in protest against this and defence spending, followed by Harold Wilson and John Freeman.
The Labour Party is then plunged into a decade of infighting between the Bevanite Left and the Gaitskellite Right (Timmins N, 2001, The Five Giants: A biography of the welfare state. HarperCollins).
The report, The work of nurses in hospital wards: Report of a job analysis, is published by the Nuffield Provincial Hospitals Trust.
Following three years of research, H.A. Goddard reports on perhaps the first serious study of nursing workload in the UK (Goddard HA, 1953, The work of nurses in hospital wards: Report of a job analysis. Nuffield Provincial Hospitals Trust). It is to form the basis of many studies that follow.
3.21% UK spending on the NHS as a share of GDP
Image credit: Public Health Image Library, #8954, CDC/Barbara Jenkins, NIOSH.
August 1954
The Bradbeer Committee publishes a report on the internal administration of hospitals for the Central Health Services Council.
The resulting guidance is supportive of the system typical in voluntary hospitals (which avoids the hierarchy of local authority hospitals). It draws on the former’s concept of a ‘tripartite administration’ of medical, nursing and lay elements, but with the lay element (in the person of the group secretary) given overall responsibility for implementing policy and coordinating the activities of the group.
(Watkin B, 1975, Documents on Health and Social Services: 1834 to the present day. Methuen Young Books.)
A wide-ranging review of the role of general practice encourages the formation of independent GP group practices.
The uneven distribution of primary care services was a key problem at the formation of the NHS and successive surveys demonstrated that many areas were ‘under doctored’.
In 1950, the Ministry of Health commissions Sir Henry Cohen to undertake a wide-ranging review of general practice. This leads to the provision of interest-free loans (backed by the Treasury) to help GPs develop their practice premises as well as mechanisms to control the geographical distribution of GPs.
2.87% UK spending on the NHS as a share of GDP
Image credit: Public Health Image Library, #8953, CDC/Barbara Jenkins, NIOSH.
“What is most needed at the present time is the prospect of a period of stability.”
RH Turton, Minister of Health, House of Commons Debate, 25 January 1956, vol 548, cols 207–10.
January 1956
The report of the Guillebaud Committee’s inquiry into the cost of the NHS is published. The report lays to rest many fears that the service is extravagant or cannot be afforded.
In February 1953, the Treasury requests an inquiry into the NHS and related expenditure, and the Guillebaud Committee is set up. Supported by the London School of Economics and Brian Abel Smith, the emphasis of the subsequent report is intended to be on preventing further increases in expenditure, rather than introducing cuts.
However, the Guillebaud Report finds that: in relative terms, NHS spending had fallen between 1948 and 1954, from 3.75 per cent to 3.25 per cent of Gross National Product; that capital spending was running at only 33 per cent of pre-war levels; and that additional costs implied by an ageing population could be financed easily by economic growth.
2.88% UK spending on the NHS as a share of GDP
“Co-operation between general practitioners and health visitors... is lacking in many cases at the moment.”
The Jameson Working Party report on health visiting is published.
Following repeated attacks by the social work and medical professions, a Working Party is set up to try to work out a clearer picture of what health visitors could and should not be doing, amidst concern that their work intrudes on the roles of other groups.
In its recommendations, it suggests a role that would combine basic health education with concern for signs of social dysfunction.
2.90% UK spending on the NHS as a share of GDP
July 1956
The Clean Air Act is enacted by Parliament in response to worsening air pollution in urban areas of the UK.
The Clean Air Act is enacted by Parliament in 1956 as a response to high mortality rates during the Great Smog of 1952 and to the Beaver Committee Report that was commissioned in its aftermath.
The Act aims to control domestic sources of smoke pollution by introducing smokeless zones in which homes and business can only burn smokeless fuels.
Willink’s Report of the Committee to consider the future numbers of medical practitioners and the appropriate intake of medical students is published.
In response to the growing number of specialist registrars unable to secure consultant posts, a committee is set up under Henry Willink to examine the supply of medical professionals.
The committee concludes that too many doctors are being trained and proposes a 12 per cent reduction. This is soon realised to be a misjudgement and in 1961 the Minister of Health is forced to increase the number of training places by 10 per cent.
The Willink Report was believed in retrospect to be responsible for the severe shortage of junior medical staff throughout the 1960s.
2.90% UK spending on the NHS as a share of GDP
Image credit: Public Health Image Library, #8990, CDC/Barbara Jenkins, NIOSH.
“Patients who are fit to live in the community... should not be in large mental institutions such as the present mental and mental deficiency hospitals.”
The report of the Royal Commission on Mental Illness and Mental Deficiency, a response to widespread concern about the care of people with mental illness and the first step towards community care, is published.
In 1954, a Royal Commission, chaired by Lord Percy, is instructed to enquire into “the existing law and administrative machinery governing the certification, detention, care... absence on trial, or licence, discharge and supervision of persons who are or allege to be suffering from mental illness or mental defect” (Royal Commission terms of reference).
The Commission’s report, published in 1957, calls for the abolition of special legal formalities connected with mental illness and mental deficiency; the absorption of mental health in the general administration of the NHS; and the extension of local authorities’ powers and duties (Jones K, 1972, A history of the mental health services. Routledge & Kegan Paul, p.306).
Mental health problems go on to form the largest category of spending in the NHS.
2.90% UK spending on the NHS as a share of GDP
July 1959
The Mental Health Act replaces much of the existing legislation on the provision of mental health services in England, bringing the provision of mental health services within the general administrative machinery of the NHS for the first time.
Building on the conclusions of the Percy Commission, the Mental Health Act 1959 enshrines two principles in law: the provision of as much treatment as possible on a voluntary and informal basis; and a new system of safeguards in cases where compulsion is necessary (Jones K, 1972, A history of the mental health services. Routledge & Kegan Paul, p.307).
In so doing, the Act also oversees the closure of large psychiatric hospitals in favour of community-based services.
The Report of the Royal Commission on Doctors’ and Dentists’ Remuneration is published.
Pay is poor, particularly for GPs, and often based on pre-war values. Emigration is increasingly common.
The Royal Commission is appointed in March 1957 to settle an ongoing dispute between the medical profession and the Government over pay, which even leads to the Conservative Government planning for a ‘phased withdrawal’ from the NHS.
It attempts to reach a formula that would satisfy both parties and publishes its recommendations in 1960. A key recommendation is the creation of an independent review body system for deciding NHS doctors’ and dentists’ pay.
“We have to strive to alter our whole mentality about hospitals and mental hospitals especially. They stand isolated, majestic, imperious, brooded over by the giant water tower and chimney combined, rising unmistakable and daunting out of the countryside"
Enoch Powell (1961) Water Tower Speech, quoted on studymore.org.uk
March 1961
Enoch Powell makes his ‘Water Tower’ speech
Having seen the statistics of the falling numbers of patients in mental hospitals as a result of drug treatment, Powell proposes the closure of large asylums and provision of more local care.
3.05% UK spending on the NHS as a share of GDP
July 1961
The Human Tissue Act issues guidance on the use of the bodies of deceased persons for medical or educational research, stating that professionals must have no reason to believe that any surviving relatives object.
“This plan... will provide for patients... an environment which will challenge comparison with that available anywhere in the world.”
Enoch Powell, Minister of Health, House of Commons Debate, 4 June 1962, vol 661, cols 31–160.
June 1962
Enoch Powell’s Hospital Plan recommends the development of district general hospitals covering populations of around 125,000.
Enoch Powell is an enthusiastic sponsor of the Hospital Plan, which he describes as “an opportunity to plan the hospital system on a scale which is not possible anywhere else certainly on this side of the Iron Curtain”.
The objective is to remedy a decade of neglect, closing many hospitals and replacing them with new or extended facilities.
£570 million is pledged over 10 years to provide a national network of district general hospitals throughout the UK. Although this proved to be an underestimate of the costs involved, the hospital plan provided a road map for strategic planning as resources gradually became available.
3.00% UK spending on the NHS as a share of GDP
“We have concluded that in future one administrative unit should become the focal point for all the medical services of an appropriate area.”
Porritt Committee, quoted in British Medical Journal (1962) ‘Porritt report on N.H.S.’ British Medical Journal 2, 1171–3.
November 1962
The Medical Services Review Committee’s final report (the Porritt Report) is published.
In November 1958, the Medical Services Review Committee, chaired by Sir Arthur Porritt, President of the Royal College of Surgeons and of the British Medical Association, is backed by all the major British medical bodies to assess the provision of health services in England and Wales.
Porritt’s final report suggests reforming the tripartite structure by transferring the responsibility for the administration and coordination of all medical and ancillary services in any given area into the hands of one authority – namely an area health board.
3.0% UK spending on the NHS as a share of GDP
March 1965
The Family Doctors Charter asks for changes to make the provision of a good service easier, by subsidising premises and staffing and improving pay and working hours.
By the early 1960s, GPs are complaining of neglect and impoverishment. Morale is poor and recruitment is proving difficult. The mounting crisis leads to the Family Doctors Charter, which receives widespread support from the profession (including the threat of 18,000 resignations if it is not implemented).
Following further negotiations with the Government, key aspects of the charter are incorporated into the second major iteration of the GP contract.
With falling GP morale, the negotiations on the Charter for General Practice provide financial incentives for practice development, plus substantial rewards.
A milestone in defining the role of general medical services, the 1966 GP contract addresses major grievances of GPs and provides for better-equipped and better-staffed premises, greater practitioner autonomy, a minimum income guarantee, and pension provisions.
3.50% UK spending on the NHS as a share of GDP
March 1967
The Cogwheel Report examines the organisation of doctors in hospitals.
In order to address the mistrust between doctors and hospitals, the report recommends that doctors become more deeply involved in medical management. The formation of medical divisions along clinical lines is also proposed in order to encourage better methods of medical practice and financial management.
The Abortion Act legalises abortions up to 28 weeks’ gestation for all women, not only when the life of the mother is in danger as was previously the law.
“A community based and family oriented service, which will be available to all.”
Seebohm Report, quoted in Donnison DV (1969) ‘The Seebohm Report and its implications’ International Social Work 12, 11–17.
March 1968
The Report of the Committee on Local Authority and Allied Personal Social Services is published.
With an ambition to save costs and resources, the Seebohm Committee recommends the integration of children, elderly and mental welfare services into one family services department.
Following the publication of these recommendations, social services departments are established in local authorities, creating a division between health and social services that persists to this day.
3.65% UK spending on the NHS as a share of GDP
July 1968
The publication of Kenneth Robinson’s Green Paper, Administrative structure of the medical and related services in England and Wales, presages years of argument about the organisational structure of the NHS. A major issue throughout is the relationship between the NHS and local authorities, and health and social care.
Robinson was instructed to explore possible changes to the NHS administration by the then Prime Minister, Harold Wilson, following numerous criticisms of its tripartite structure and other organisational deficiencies.
The Green Paper recommends the creation of about 50 area boards in a single organisational tier, taking responsibility for all health functions in each administrative area.
3.57% UK spending on the NHS as a share of GDP
Public Health Image Library, #12433, CDC.
September 1968
The Ministry of Health merges with the Ministry of Social Security to form the Department of Health and Social Security.
In response to the growing chasm between the NHS and social care provision, the Ministry of Health is merged with the Ministry of Social Security to form the Department of Health and Social Security.
Kenneth Robinson is moved to the Ministry for Planning and Land, and Richard Crossman is made Secretary of State for Health and Social Security.
“Our basic purposes are to unite the National Health Service and to integrate its separate services locally.”
Baroness Serota, Minister of State, Department of Health and Social Security, House of Lords Debate, 11 Feb 1970, vol 307, cols 899-903.
February 1970
Crossman re-writes Robinson’s proposals in the second Green Paper on the NHS.
Partly in response to criticisms of Robinson’s 1968 plan, Richard Crossman makes extensive revisions to the first NHS Green Paper, leading to the publication of the second Green Paper on the NHS.
Crossman rejects the idea of local authorities managing the health service, proposing instead that area authorities should remain directly accountable to the Department of Health and Social Security.
But he retains the idea that the number and areas of the new health authorities should match those of the new local authorities, adding that regional health councils could undertake those activities for which the areas are too small.
3.46% UK spending on the NHS as a share of GDP
“Our proposals for the new NHS offer a great, and indeed a new, opportunity for a partnership with local authorities.”
Sir Keith Joseph, Secretary of State for Social Services, House of Commons Debate, 1 Jul 1971, vol 820, cols 591-657
July 1971
The Conservatives revise Crossman’s plan for reform following their election in 1970, with major management consultant involvement, coterminosity and consensus management being introduced.
Following the surprise Conservative victory in 1970, the new Secretary of State for Social Services, Sir Keith Joseph, puts out a new consultative document amending Crossman’s 1970 proposals.
The consultation proposes that new regional health authorities should be responsible for general planning and allocation of resources to area health authorities, as well as the coordination and supervision of the latter’s activities.
3.65% UK spending on the NHS as a share of GDP
June 1972
Launch of the Cochrane report.
A.L. Cochrane’s seminal report, published in 1972, set out the vital importance of randomised controlled trials (RCTs) in assessing the effectiveness of treatments.
Cochrane’s pioneering text revolutionised policy making and the delivery of health care as we know it today, and the full legacy of his work was celebrated in a 25th anniversary report written by Alan Maynard for the Nuffield Trust in 1997.
3.64% UK spending on the NHS as a share of GDP
Nuffield Trust
July 1973
NHS reorganisation: after years of debate, structural changes are made in the NHS Reorganisation Act.
In an effort to generate better coordination between health authorities and local authorities, the NHS Reorganisation Act sees the traditional tripartite structure replaced by a unitary structure with 90 health authorities reporting to 14 regional health authorities. Under the reforms, regional, area and district heath authorities replace regional hospital boards, taking over public health and other services from local authorities in the process.
The highly prescriptive Management arrangements for the reorganised NHS (1972), known as the ‘Grey book’, recommends a system of consensus management, with detailed role specifications for all NHS officers.
3.68% UK spending on the NHS as a share of GDP
Conservative politician Sir Edward Heath, Prime Minister at the time of the NHS Reorganisation Act.
“The recommendations will certainly simplify the pay structure.”
British Medical Journal (1974) ‘Overdue recognition for nurses’ British Medical Journal 3, 762.
September 1974
The Halsbury Committee on the pay and conditions of nurses and midwives awards pay increases of up to 40 per cent.
The review highlights the "complexity of staffing" and pay structures, and recommends that the grading and pay structure for nurses and midwives be integrated. Also notable is recognition of the ward sister role, holders of which it is argued deserve extra remuneration.
4.17% UK spending on the NHS as a share of GDP
June 1975
The Merrison Report suggests that the General Medical Council (GMC) should become responsible for regulating postgraduate medical education and training and hold a list of all registered specialists and GPs. These recommendations are not implemented but the report does lead to the creation of the Education Committee of the GMC.
The Merrison Report proves a key shaper of the Medical Regulation Act 1978, which makes the GMC more accountable, extends its functions – particularly in relation to medical education – and separates the disciplinary processes from those that deal with doctors whose performance is impaired by ill-health.
4.52% UK spending on the NHS as a share of GDP
Public Health Image Library, # 3605, CDC/ Va. McPheeters.
“Health care is for people and clearly the primary determinant of need must be the size of the population.”
Department of Health Resource Allocation Working Party (1976) Sharing resources for health in England: Report of the Resource Allocation Working Party. Department of Health.
September 1976
Sharing resources for health in England: Report of the Resource Allocation Working Party is published.
The report is the first systematic attempt to address the major inequity between health spending in London and the south east of England and the much lower levels - broadly half - spent elsewhere in the country. RAWP proposes using mortality in each area as an indicator of health care need.
The formula is in use from 1977 to 1990 and gradually manages to redistribute resources from the metropolitan regions to the poorer regions in the north.
4.40% UK spending on the NHS as a share of GDP
September 1978
Access to basic health care is affirmed as a fundamental human right in the Declaration of Alma-Ata, which leads to the World Health Assembly setting specific targets in the report Achieving health for all by 2000.
at least five per cent of Gross National Product to be spent on health;
at least 90 per cent of children to have a weight for age that corresponds to the reference values;
safe water should be available in the home or within 15 minutes’ walking distance and adequate sanitary facilities should be available in the home or immediate vicinity;
people should have access to trained personnel for attending pregnancy and childbirth; and
child care should be available up to at least one year of age.
The NHS’s financial problems worsen during the winter of 1978–79 as a result of the oil crisis. Widespread strikes are prompted across Britain following attempts to impose a pay freeze to control inflation.
4.08% UK spending on the NHS as a share of GDP
James Callaghan, British Prime Minister, 1976 to 1979.
A Conservative election victory, plus the Royal Commission on the NHS reports that while there are concerns that include an ageing population and the cost of technological developments, the NHS is in no danger of collapse.
Undermined by a change in Government, among the 117 recommendations made by the Commission are: compulsory wearing of seat belts for the driver and front seat passenger of a motor vehicle; health departments to be encouraged to experiment with their budgets; and the gradual extinction of charges in the NHS.
3.96% UK spending on the NHS as a share of GDP
1980s
March 1980
The London Health Planning Consortium reports are published.
A series of reports by the NHS in London and the University of London (Lord Flowers) are published on an appropriate pattern of hospital service and medical schools for London. It was a spur to the amalgamation of some hospitals and trusts, to provide larger units for medical education and specialist services, e.g. UCH and the Middlesex hospitals and medical school.
“The crude differences in mortality rates between the various social classes are worrying.”
Secretary of State for Social Services, David Ennals, 1977, quoted in Levitas R and Guy W eds (1996) Interpreting official statistics. Routledge.
August 1980
The Black Report shows health inequalities persist.
The Black Report is commissioned by Labour but published by the Conservatives and given only limited circulation. It shows not only that inequalities exist but also that the gap is widening. In spite of Government policies, health inequalities persist.
4.46% UK spending on the NHS as a share of GDP
“The Acheson report emphasised low cost, feasible solutions.”
The Acheson Report on primary health care in inner London is published.
After this report, it becomes impossible to consider hospital service changes without taking primary care into account.
4.45% UK spending on the NHS as a share of GDP
October 1982
The Körner Steering Group on Health Services Information, established in 1980, reports and builds on existing data systems to improve their usefulness for management.
The Steering Group recommends developing a set of basic statistics that every health authority would have to produce. Concerns are raised about the cost and management resources needed to set up this NHS data model for the first time. It is implemented in 1987, in the same year as a Committee for Regulating Information Requirements is established.
NHS reorganisation: NHS restructuring abolishes area health authorities (AHAs).
In 1982, the area tier of NHS management is abolished, resulting in 192 district health authorities (DHAs) that are responsible to the regional health authorities. The aim is to simplify the structure. However, this was to be the start of many future reorganisations of health authorities over the next three decades.
“If Florence Nightingale were carrying her lamp through the corridors of the NHS today, she would almost certainly be searching for the people in charge.”
Griffiths Report, 1983, quoted in Attwood M and Beer N (1988) ‘Development of a learning organisation – reflections on a personal and organisational workshop in a district health authority’ Management Learning Journal 19(3), 201–14.
February 1983
The Griffiths Report introduces general management to the NHS and heralds a major increase in managers' pay.
The Griffiths Report enshrines the general management function, removing the consensus management system of 1974 that is widely regarded as having failed. It was an attempt to ensure that someone was in charge and could be held accountable. It leads to a major increase in managers' pay.
4.40% UK spending on the NHS as a share of GDP
May 1983
The Mental Health Act 1983 legislates for the detention of people deemed to be mentally ill and a risk to themselves or others, with or without their consent.
The Mental Health Act allows individuals who are assessed as being mentally ill and a risk to themselves or others, to be detained in hospital and given treatment.
This is possible without patient consent for a certain period of time and with the consent of a relative thereafter. Much of the criticism of the Act is focused on patients’ rights and the difficulties of appeal.
Due to developments in in vitro fertilisation (IVF) and embryology, a committee is formed to establish regulatory principles. This leads to the publication of the Warnock Report.
The Warnock Report leads to the Human Fertility and Embryology Act 1990, which states, among other things, that embryos can only be used for specific research purposes.
This is regulated by the Human Fertilisation and Embryology Authority, which decides on a case-by-case basis whether to allow the research.
4.30% UK spending on the NHS as a share of GDP
January 1985
Reflections on the management of the National Health Service, by Professor Alain Enthoven for the Nuffield Trust, contributes to the NHS reform programme.
In the report commissioned by the Nuffield Trust, Enthoven observes that the NHS is ‘gridlocked’ by the number of actors, issues and processes that stifle change.
He suggests that innovations to drive change should be treated as opportunities and nurtured rather than criticised or politicised.
Enthoven concludes that it is necessary to create an environment that encourages quality and efficiency improvements.
Project 2000 introduces major reform of nurse training
Project 2000 represented a major shift from an apprenticeship style of nurse training, in which a student nurse was a hospital employee, to a system where student nurses were supernumerary, spending part of their time in higher education, and part on clinical placement. It paves the way for undergraduate nurse education in subsequent decades.
The controversial Green Paper on primary care – Neighbourhood nursing: A focus for care (the Cumberlege Report) – and policy statements from the Royal College of General Practitioners, become building blocks for the reform of primary health care.
The Green Paper sparks a fierce debate on the future of primary care . Among other points, the Paper suggests extra payments to GPs who offer specific services and the creation of integrated health care shops – inspired by Health Maintenance Organisations in the United States. Both ideas make it to the White Paper in 1987 and remain prominent themes in the debate about primary care.
“The Government has at last responded... to the representations we have made to improve primary care.”
Dr Michael Wilson, chairman of the General Medical Services Committee, quoted in the British Medical Journal, 5 Dec 1987.
December 1987
The White Paper, Promoting better health, suggests improvements in patient choice and the widening of services provided by pharmacists and nurses.
This White Paper forms the basis for the new GP contract in 1990, which sets out quality and financial incentives to improve the processes of delivering care, with extra pay for undertaking health promotion, screening and other preventative actions. It leads to major increases in the skills and size of primary health care teams.
It also aimed to introduce medical audit into hospitals and primary care, and introduced Trusts for hospitals with a proven ability to manage themselves, who were given greater freedoms.
4.16% UK spending on the NHS as a share of GDP
January 1988
Prime Minister Margaret Thatcher makes the surprise announcement of an NHS review on the television programme Panorama.
3.92% UK spending on the NHS as a share of GDP
Image credit: Wikimedia Commons
“The point of all our proposals is to produce a better NHS, providing the type and standard of service a patient has a right to expect.”
Kenneth Clarke, Secretary of State for Health, House of Commons Debate, 7 November 1989, vol 159, cols 556–9W
January 1989
Split between purchasers and providers of care proposed.
The White Paper, Working for patients (NHS reforms), proposes to introduce a split between purchasers and providers of care, GP fundholders and a state-financed internal market, in order to drive service efficiency.
3.85% UK spending on the NHS as a share of GDP
1990s
April 1990
The new GP Contract provides incentives for more health promotion and to provide better care for patients.
Both the GP contract and the Hospital contract resulted in substantial increases in salaries and pay, swallowing much of the money the government had allocated to the improvement of the NHS.
NHS reorganisation: Creation of an internal market is facilitated through the National Health Service and Community Care Act 1990.
The NHS and Community Care Act 1990 creates an internal market and a purchaser-provider split in which the purchasers (mainly health authorities) are handed budgets to purchase services from providers (mainly acute hospitals and those providing care for people with mental health problems, people with learning disabilities as well as older people).
One of the most significant reforms is to establish ‘GP fund-holding’, which enables GPs to take on budgets and purchase services from hospitals and other providers on behalf of their patients.
Not all GPs become fundholders, with non-fundholders having their services purchased for them by local health authorities. Critics accuse the Government of creating a two-tier system in which patients of GP fundholders are able to access treatment more quickly than those belonging to non-fundholding GPs. Supporters of the policy claim that fundholding helps to deliver more efficient care.
The Abortion Act is replaced by the Human Fertilisation and Embryology Act. It states that abortion is no longer legal after 24 weeks except if: the mother’s life is in danger; there is extreme foetal abnormality; or there is a grave risk of physical or mental injury to the mother.
A further reduction in the number of weeks is debated in Parliament in 2008 but no changes are implemented.
4.00% UK spending on the NHS as a share of GDP
June 1991
The 1991 White Paper, Health of the nation, identifies a number of important areas for improving health, including cancer, coronary heart disease, mental health and HIV/AIDS.
“Every household should know its rights under the NHS.”
Secretary of State for Health, William Waldegrave, 5 November 1991
November 1991
The Patient’s Charter stresses the patient as a customer with rational expectations.
Secretary of State for Health, William Waldegrave, House of Commons, oral answers to questions: Health, 5 November 1991.
The Patient’s Charter outlines the rights of patients regarding the receipt and quality of service they should expect to receive.
The Charter includes specific targets for waiting times for hospital treatment. The year 1994 then sees the introduction of provider performance tables based on these targets.
4.33% UK spending on the NHS as a share of GDP
“It is essential that work be put in hand now to plan for a more appropriate level of capacity.”
Report of the inquiry into London’s health service, medical education and research (Tomlinson Report) (1992)
February 1992
The Tomlinson Report into London’s health services attempts to defuse major political dissent about the future of much-loved and ancient hospitals.
The report by Sir Bernard Tomlinson, a distinguished neuropathologist, was another step in the recurrent campaign to rationalise hospital and medical school provision in London.
After an intensive year of investigation that involved interviews with more than 1,000 health professionals and others, Tomlinson recommends the closure of Charing Cross, University College/Middlesex and St Bartholomew’s hospitals, the merger of Guy’s and Thomas’ and the closure of ten smaller hospitals. Although the government accepts most of the report, these headline recommendations are not implemented, with the exception of the eventual closure of the Middlesex. His recommendations on reducing in bed numbers, changes in specialty mix; and providing high technology services such as cardiac surgery in larger units do proceed.
4.65% UK spending on the NHS as a share of GDP
May 1992
The White Paper, The Health of the nation, targets improvement in five key areas.
The White Paper identifies coronary heart disease (CHD), cancer, mental health, AIDS/HIV and sexual health, and accidents, as five key areas for improvement. There is also some emphasis on individual responsibility for health.
Labour comes to power and publishes the White Paper, The new NHS: Modern, dependable.
The White Paper, The new NHS: Modern, dependable, led by Frank Dobson, aims to replace the internal market and GP fundholding with a more cooperative, integrated system while retaining the purchaser–provider split. Organisational change is foreshadowed.
4.64% UK spending on the NHS as a share of GDP
“The unacceptable variations that have grown up in recent years must end.”
The National Institute for Health and Clinical Excellence (NICE) is established.
The consultation document, A first class service, leads to the creation of NICE and the Commission for Health Improvement. The two new organisations aim to provide guidance on the use of technology and how to strengthen quality.
4.69% UK spending on the NHS as a share of GDP
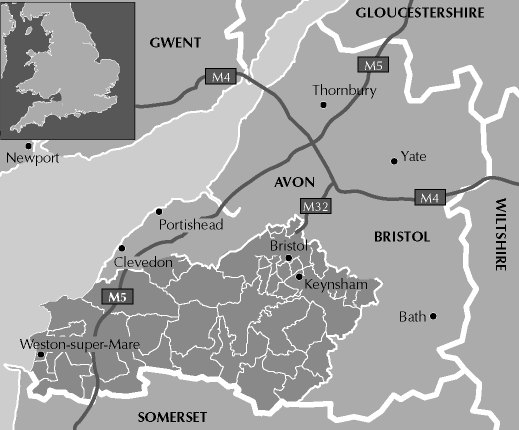
“There are no quick fixes, but progress is possible and can be achieved.”
A public inquiry is announced to understand the failings of the Bristol Royal Infirmary in providing care to children receiving cardiac surgical services.
As a result of the public inquiry, led by Professor Ian Kennedy, an increasing emphasis is placed on quality, with outcomes increasingly seen as important to contracting and the provision of care.
4.69% UK spending on the NHS as a share of GDP
“Inequalities by socioeconomic group, ethnic group and gender can be demonstrated across a wide range of measures of health and the determinants of health.”
The Acheson inquiry signals the Labour Government’s focus on health inequalities. Revised targets for reducing infant mortality and increasing life expectancy at birth are set out in Public Service Agreements between the Department of Health and the Treasury.
4.69% UK spending on the NHS as a share of GDP
“NHS Direct is here to make a difference to the lives of people in England, 24-hours a day, 365 days a year.”
What is NHS Direct? on www.nhsdirect.nhs.uk.
December 1998
NHS Direct is established.
NHS Direct, a national health line providing expert health advice and information, is established.
4.69% UK spending on the NHS as a share of GDP
March 1999
The Royal Commission on Long Term Care reviews the options for the ongoing funding of long-term care of older people.
The Royal Commission recommends that all nursing and personal care provided in nursing homes and in people’s homes should be free. Two members of the Commission, Lord Lipsey and Lord Joffe, co-author a minority report that opposes the case made by the majority of the Commission for free personal care for all, financed from taxation.
When the Government responds with The NHS Plan in 2000, a reduced version of this is implemented with nursing care to be provided free of charge, but with personal care remaining means tested. Scotland becomes the only country in the UK to offer free personal and nursing care at home.
4.73% UK spending on the NHS as a share of GDP
“We are putting forward the first comprehensive Government plan focused on the main killers: cancer, coronary heart disease and stroke, accidents, mental illness.”
The Labour Government’s White Paper, Our healthier nation, follows up on a previous paper by the Conservatives in 1992.
Our healthier nation outlines targets for improving public health, with a new focus on health inequality and the economic, social and environmental causes of ill-health.
It aims to increase healthy life expectancy and narrow the health gap. A Minister for Public Health is appointed.
4.73% UK spending on the NHS as a share of GDP
“Bringing the NHS back to the people and ensuring that the staff work together instead of fighting among themselves.”
Laura Moffatt MP, House of Commons, oral answers to questions: Health Bill, 13 April 1999.
April 1999
NHS reorganisation: GP fundholding is abolished; new primary care groups (PCGs) are established.
GPs, nurses and other workers come together under a new system of primary care groups (PCGs) to commission care on behalf of their local communities. The Government claims that the reforms will lead to patients having closer contact with the professionals that decide what treatments they can have. Around 500 PCGs – controlling the majority of the NHS budget – are due to be created.
4.73% UK spending on the NHS as a share of GDP
2000s
January 2000
The most expensive breakfast.
Interviewed on Breakfast with Frost, an early morning television programme, Tony Blair made an apparently impromptu and uncosted promise to raise spending on the NHS to the average European spend
The NHS Plan – a 10-year modernisation programme of investment and reform.
The NHS Planoutlines a strategy for more doctors, more nurses, more beds and 100 hospital building schemes by 2010, with improved access to hospitals and primary care and a renewed focus – through performance targets – on decreasing waiting times.
A new model of financing is agreed: instead of public money, the Private Finance Initiative takes loans at high interest rates to design, build and operate hospitals building up huge commitments on future revenues. The Plan also sets out revised targets for issues such as waiting times.
As directed by the Health Act 1999, the Commission for Healthcare Improvement is created – the first organisation to formally assess the performance of NHS hospitals.
May 2001
The Health and Social Care Act 2001 formalises The NHS Plan.
“This is the first time we have assessed performance on issues that patients care about.”
John Hutton, Minister of State, Department of Health, Westminster Hall debates, 28 November 2001
September 2001
Introduction of the hospital star rating system.
The first of a series of attempts to measure and publicise the quality of care delivered by hospitals, the hospital star rating system is modified each year and ends up being scrapped in 2005.
5.25% UK spending on the NHS as a share of GDP
“All our efforts need to be focused on supporting front line staff to deliver these improvements and empowering them to make decisions locally.”
NHS reorganisation: District health authorities are replaced by strategic health authorities (SHAs) and primary care trusts (PCTs). The concept of foundation trusts is investigated.
The White Paper, Shifting the balance of power, sees the abolition of 95 health authorities, which are partly replaced by primary care groups (PCGs) and trusts and by 28 strategic health authorities (SHAs), to provide regional management for the NHS and oversee the work of primary care trusts (PCTs).
303 PCTs are established and given responsibility for approximately 80 per cent of the NHS budget. Mergers soon halve the number.
5.53% UK spending on the NHS as a share of GDP
“The Review flags the need for a very substantial increase in resources for health and social care.”
Published in April 2002, his report suggests that future funding needs will depend on the extent to which future demand for health care is reduced by good public health policies and by disease prevention.
The report justifies what is to be a 50 per cent real-terms increase in NHS spending over the five years after its publication.
5.53% UK spending on the NHS as a share of GDP
June 2002
The National Health Service Reform and Health Care Professions Act 2002 legislates for the redistribution of power from regional health authorities into strategic health authorities (SHAs).
The National Health Service Reform and Health Care Professions Act 2002 also includes a duty to create consultative patients’ forums within each primary care trust (PCT) and NHS trust. A Council for the Regulation of Health Care Professionals is formed to provide advice, conduct investigations and encourage professionals to work together.
5.53% UK spending on the NHS as a share of GDP
June 2003
New contracts for GPs and hospital consultants are agreed, changing the delivery of services to patients.
A new contract for GPs is negotiated, resulting in: more autonomy for practices about the range of services they provide; the ability to cease providing 24-hour care; and supplementary pay for reaching standards set out in the Quality and Outcomes Framework.
The new contract increases wages and pensions. Hospital consultants’ contracts are also renegotiated with the aim of increasing the amount of direct time spent with patients.
5.92% UK spending on the NHS as a share of GDP
“The new NHS/HPSS pay system is based on the principle of equal pay for work of equal value.”
Standardisation of pay and conditions for the majority of NHS staff as part of the Agenda for Change.
In exchange for pay increases, the majority of NHS staff vote in favour of the Agenda for change, which aims to modernise the NHS, for example by introducing operating theatres that remain open 24/7.
It is also hoped that the change in pay and conditions will help to increase the recruitment and retention of staff in the NHS.
5.92% UK spending on the NHS as a share of GDP
November 2003
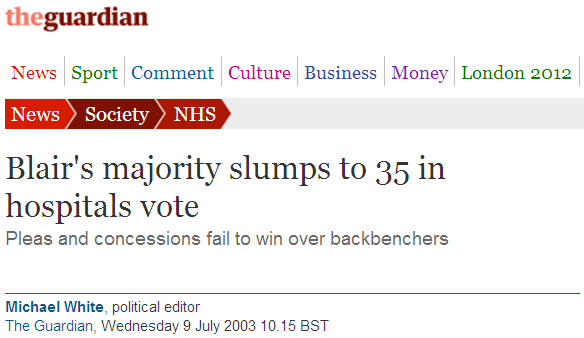
NHS reorganisation: The Health and Social Care (Community Health and Standards) Act 2003.
This Act provides for the establishment of NHS foundation trusts, semi-autonomous acute trusts with greater freedoms; two new inspectorates – the Commission for Healthcare Audit and Inspection and the Commission for Social Care Inspection; and the recovery of NHS charges.
The introduction of foundation trusts is opposed by many Labour MPs and the legislation has to survive one of the largest revolts of Tony Blair’s premiership, with as many as 65 Labour MPs voting against the reforms during the Bill’s passage.
5.92% UK spending on the NHS as a share of GDP
Image credit: The Guardian (9 July 2003).
“NHS foundation trusts are firmly part of the NHS and subject to NHS standards, performance ratings and systems of inspection.”
The first 10 foundation trusts (FTs) are established, with more control over their budgets and services.
April 2004
The Healthcare Commission takes over from the Commission for Healthcare Improvement.
October 2004
The Government outlines plans for involving GP practices in commissioning health care services through its ‘practice based commissioning’ policy
While the concept of practice based commissioning had been outlined in the 1998 White Paper, The new NHS, and in the NHS Improvement Plan in June 2004, this paper outlines in more detail how those GP practices wishing to do so will be given indicative commissioning budgets. The reforms are announced as part of the Government’s plans to devolve responsibility for commissioning services from PCTS to local GP practices.
6.26% UK spending on the NHS as a share of GDP
Information source: iStockphoto #18570063.
“We are clear that Government cannot – and should not – pretend it can ‘make’ the population healthy. But it can – and should – support people in making better choices for their health.”
The Government’s public health White Paper, Choosing health, is published.
The public health White Paper, Choosing health, reiterates the agenda to promote individual responsibility with a focus on issues such as smoking, obesity, diet and nutrition, exercise and sexual health.
The White Paper supports individual choice, personalised services and coordinated working between the public and private sectors.
6.26% UK spending on the NHS as a share of GDP
July 2005
The Government accelerates the timetable for the introduction of practice-based commissioning through the publication of the report: Commissioning a patient-led NHS.
The document outlines plans to: better engage local clinicians in the design of services; roll-out practice-based commissioning universally and to a faster timetable; develop primary care trusts (PCTs) to support practice-based commissioning; and to review the functions of strategic health authorities (SHAs) to support commissioning and contract management.
The document instructs PCTs to “make arrangements for 100 per cent coverage of practice-based commissioning by no later than the end of 2006”, although individual practices are given some flexibility to take on commissioning to a greater or lesser extent depending on their wishes and capabilities.
All budgets are set to be ‘indicative’ only, with PCTs continuing to hold the actual funds.
NHS reorganisation: Strategic health authorities (SHAs) are reduced from 28 to 10. The number of primary care trusts (PCTs) falls from 303 to 152.
The organisation of the NHS is continually changing and PCTs frequently merge to reduce overhead costs, reducing their ties to specific individual communities in the interests of efficiency.
6.38% UK spending on the NHS as a share of GDP
“Services that are flexible, integrated and responsive to peoples’ needs and wishes.”
The White Paper, Our health, our care, our say, is published.
The White Paper encourages patient choice and the movement of services out of hospitals into community services.
6.38% UK spending on the NHS as a share of GDP
June 2007
The Conservative Party outlines its vision for the future of the NHS in the White Paper: NHS autonomy and accountability: Proposals for legislation.
Under the proposed reforms, Shadow Health Secretary Andrew Lansley outlines plans to: scrap the NHS ‘targets culture’; reduce red tape; give patients the power to decide how they should be treated; hand day-to-day control of the NHS to an independent board; and put senior doctors in charge of local budgets with power to decide how NHS money is spent.
If elected, the Conservatives’ policy paper also pledges that patients will be allowed to secure treatment at their hospital of choice, whether in the public or private sector, as long as it delivers care at or below the NHS cost.
A number of papers that outline the Conservatives’ policies on health in more detail are published throughout 2008 and 2009, trailing many of the NHS reforms that were to be introduced following the 2010 General Election.
6.51% UK spending on the NHS as a share of GDP
July 2007
Healthcare for London: A framework for action, a major review into the future of London’s health services, led by clinician Professor Sir Ara Darzi, is published.
Ara Darzi, an eminent clinician and later a Labour Minister, consulted widely on his proposals to take professional colleagues along with him. He took into account changing demography and population aging, the altering pattern of disease, and developments in specialist medicine
Following an invitation from David Nicholson, Chief Executive of NHS London (the London SHA), Professor Sir Ara Darzi undertakes a major review of London’s health services. His resulting report, Healthcare for London: A framework for action [pdf], sets out how London’s health care needs to change over the following 10 years.
The underlying emphasis is on moving the provision of routine health care closer to people’s homes and centralising specialist care services. Specific recommendations include the development of academic health science centres and the introduction of polyclinics – a term used to describe large community facilities that will provide a much wider range of services than is offered by most GP practices, such as minor procedures, urgent care and x-rays.
6.51% UK spending on the NHS as a share of GDP
Image credit: Wikimedia Commons
July 2007
A ban on smoking in nearly all enclosed work places and public places in England is introduced.
A smoking ban in England comes into effect, following similar measures that had already been introduced in Scotland in March 2006, Wales in April 2007 and Northern Ireland in April 2007.
6.51% UK spending on the NHS as a share of GDP
“My aim is to convince and inspire everyone working in the NHS, and in partner organisations, to embrace and lead change.”
Health Minister, Lord Darzi, leads what becomes known as the ‘NHS next stage review’ and outlines his 10-year vision for the NHS in the report, High quality care for all.
Professor Sir (soon to become Lord) Darzi joins the Government as Parliamentary Under-Secretary of State in the Department of Health and is tasked with leading a major review of the NHS to outline a 10-year vision for its future. A series of reports appears, with many clinically driven and defining good practice.
Lord Darzi’s vision includes major reconfiguration of hospital services, driven by quality and the clinical realities of where care is best delivered. Centralising specialist services is a major theme, while polyclinics (large community facilities providing a much wider range of services than is offered by most GP practices) are proposed.
6.99% UK spending on the NHS as a share of GDP
January 2009
The NHS Constitution is published, outlining a revised set of rights and responsibilities for patients and staff.
The NHS Constitution sets out seven principles on how the NHS should act and make decisions, six core values and a number of pledges to patients and staff, as well as a list of their rights and responsibilities. This includes treating patients with dignity and respect and enabling informed choice.
A new health and social care regulator, the Care Quality Commission (CQC), is created.
The CQC, a new independent regulator of all health and social care services in England, is created following the merger of three regulators: the Healthcare Commission, the Commission for Social Care Inspection and the Mental Health Act Commission.
The CQC takes on responsibility for regulating and inspecting health and social care services in England, including services provided by the NHS, local authorities, private companies and voluntary organisations. The CQC’s remit extends to protecting people whose rights are restricted under the Mental Health Act.
7.59% UK spending on the NHS as a share of GDP
June 2009
NHS Chief Executive Sir David Nicholson, warns the NHS to prepare for the need to release unprecedented efficiency savings of between £15 billion and £20 billion between 2011 and 2014.
Sir David Nicholson, writing in his 2008/09 annual report, sets the scene for future efficiency savings by warning the NHS to plan “on the assumption that we will need to release unprecedented levels of efficiency savings between 2011 and 2014 – between £15 billion and £20 billion across the service over the three years”. This figure is widely cited in subsequent debates and discussions.
The Robert Francis Inquiry report into Mid-Staffordshire NHS Foundation Trust is published.
Robert Francis QC publishes his inquiry report into Mid-Staffordshire NHS Foundation Trust, following concerns about standards of care at the Trust. Evidence from patients, their relatives and staff informs the final report, which consists of 18 recommendations. The Department of Health and the Trust Board accept the recommendations in full.
Labour publishes the White Paper, Building the National Care Service, on the future of social care funding, weeks before losing the General Election.
The Government proposes a National Care Service, which would provide services free at the point of need.
Decisions on how this would be funded are not clarified and the policy is dropped following the election of the coalition Government. However, the debate is to continue with the creation of the Commission on Funding of Care and Support in July 2010.
7.5% UK spending on the NHS as a share of GDP
May 2010
Following talks between the Conservative and Liberal Democrat negotiators, the Coalition Agreement is published.
After eight years as Shadow Secretary of State for Health, Andrew Lansley is appointed to the Cabinet, joined by a team of Conservative and Liberal Democrat junior ministers. Among many pledges on health, the Coalition Agreement promises “no more top-down reorganisations of the NHS”.
7.5% UK spending on the NHS as a share of GDP
“The events at Mid-Staffordshire were a tragic story of targets being put before clinical judgement and patient care.”
Secretary of State for Health, Andrew Lansley MP, announces a public inquiry into Mid-Staffordshire NHS Foundation Trust.
In June 2010, following the General Election, new Secretary of State for Health, Andrew Lansley MP, announces a public inquiry into Mid Staffordshire NHS Foundation Trust. The public inquiry examines the operation of the commissioning, supervisory and regulatory bodies responsible for the Trust.
7.5% UK spending on the NHS as a share of GDP
July 2010
The White Paper, Equity and excellence: Liberating the NHS, is published.
The White Paper reveals the Coalition Government’s plans for reforming the NHS in England.
Alongside significant structural change, the centre-piece of the proposals entails shifting responsibility for purchasing care to groups of GPs, whose experience in referring patients is felt to place them in a better position to identify efficiencies and demand quality from providers.
Concerns are muted at the scale and pace of the plans, with critics claiming that the changes would distract the NHS from achieving the £20 billion in productivity savings it has committed to achieving up to 2015. The White Paper paves the way for the 2012 Health and Social Care legislation.
The Government's vision for public health in England is published in Healthy lives, healthy people.
The public health strategy [pdf] proposes a new organisation – Public Health England – whose sole responsibility would be to provide advice and influence public health issues. Crucially, it also entails the return of public health back to local authorities, after more than two decades as a subset of the NHS.
7.5% UK spending on the NHS as a share of GDP
January 2011
NHS reorganisation: The Health and Social Care Bill 2010/11 proposes significant reforms to increase the influence of GPs on commissioning, increase competition and abolish strategic health authorities (SHAs) and primary care trusts (PCTs).
It envisages a bottom-up, clinically owned network of GP commissioning groups with ‘real’ budgets to buy care on behalf of their local communities; shifting many of the responsibilities historically located in the Department of Health to a new, politically independent NHS Commissioning Board; creating a health-specific economic regulator (Monitor) with a mandate to guard against ‘anti-competitive’ practices; and moving all NHS trusts to autonomous foundation trust status.
SHAs and PCTs are to be abolished, while integration between NHS and local authority services is to be strengthened through new health and wellbeing boards. The voice of patients is to be empowered through the establishment of a new national body, Health Watch, and local Health Watch organisations. Public Health England, a new body, is the lead on public health at the national level, with local authorities taking the lead locally.
Meanwhile, the landscape of health care provision is to be galvanised by a dose of competitively driven innovation, with an expectation of easier entry and exit to the market for a range of private and voluntary sector providers.
7.4% UK spending on the NHS as a share of GDP
“Under our proposed system everybody who gets free support from the state now will continue to do so and everybody else would be better off.”
Andrew Dilnot, Chair of the Commission for Funding of Care and Support, quoted on the Commission’s website.
July 2011
The Dilnot Review into the funding of adult social care calls for major reforms.
The Commission for Funding of Care and Support, chaired by economist Andrew Dilnot, is tasked with finding a way to create an affordable and sustainable funding system.
The Commission proposes a new system where means-tested support is extended but with a cap on the lifetime care costs that every individual can expect to pay. If introduced, the policy would require additional funding, the source of which is a point of debate.
7.4% UK spending on the NHS as a share of GDP
October 2011
Foundations are laid for the new architecture of the NHS.
As planned, the new NHS Commissioning Board is established as a special health authority, primary care trusts (PCTs) are clustered and begin to support new commissioning arrangements, and strategic health authorities (SHAs) reduce in number to four regional bodies.
Following nearly 18 months and thousands of amendments, the Health and Social Care Bill is passed.
Last-minute attempts to derail the Health and Social Care Bill are defeated as the Bill is passed. Medical leaders passionately opposed to the Bill urge GPs to limit the ‘worst effects’ of the legislation, while the Labour Party pledges to repeal the Bill if re-elected.
“We are not seeking preferential treatment but fair treatment. The Government’s wholesale changes to an already reformed NHS pension scheme cannot be justified.”
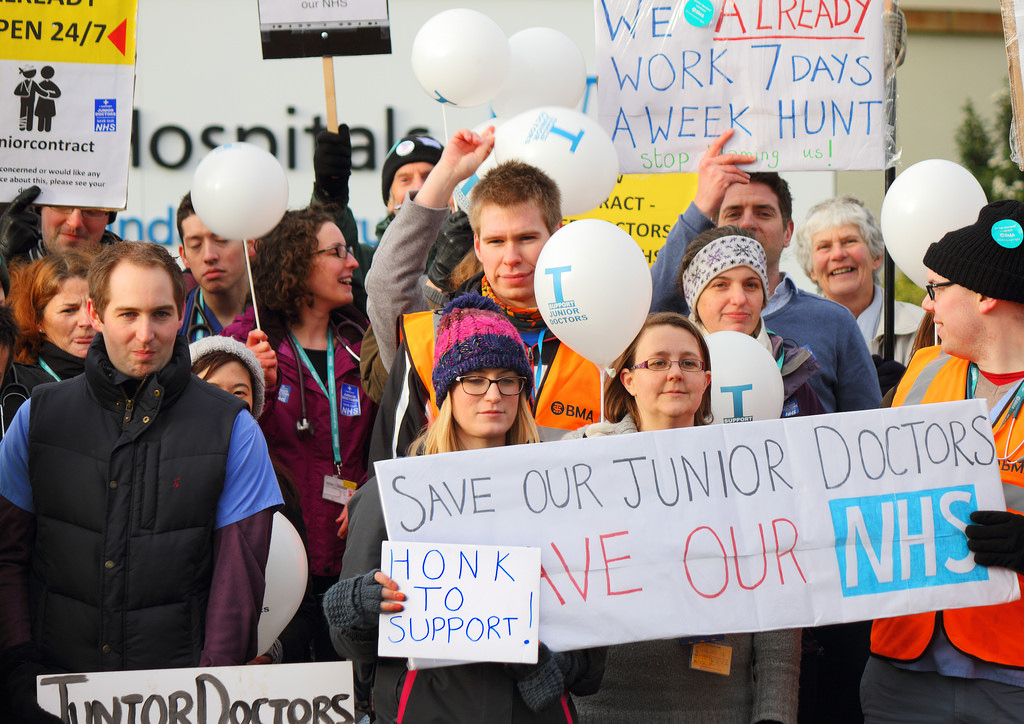
Doctors take industrial action for the first time in almost 40 years. The British Medical Association (BMA) made the decision to strike over major changes to the NHS pension scheme.
July 2012
The coalition Government publishes a Care and Support White Paper, together with a draft Care and Support Bill and a ‘progress report’ on funding, all of which outline the Government’s vision for reforming adult care and support.
Several key measures are announced in the Care and Support White Paper, together with the draft Care and Support Bill, including: access to care to be consistent through a national threshold for basic care and people to not have their care interrupted if they move around the country; carers to have new rights to public support; greater national consistency in access to care and support to be introduced; and integration of different services to be improved.
An accompanying ‘progress report’ on funding, outlines the Government’s support for the principles of the Dilnot Commission’s model, therefore financial protection through capped costs and an extended means test would be the basis for any new funding model.
Alongside this, the Government commits to introducing a Universal Deferred Payments scheme to ensure no-one will be forced to sell their home to pay for care in their lifetime. However, the Government does not commit to introducing a new system at this stage, with decisions on funding reform put back until the next Spending Review when a “final decision will be taken”.
The NHS Commissioning Board is established as an independent statutory body. However, it initially performs only limited functions. A primary role is to establish and authorise clinical commissioning groups ahead of 1 April 2013.
At the same time, Monitor starts to take on its new regulatory functions; and Health Watch England and local Health Watch bodies are established.
7.31% UK spending on the NHS as a share of GDP
Chair of Monitor, Dr David Bennett.
November 2012
As set out in the Health and Social Care Act 2012, the Government publishes objectives and expectations for the health service in its first Mandate to the NHS Commissioning Board.
The Mandate will determine the criteria on which the NHS Commissioning Board (NHSCB) will be held to account for its performance up to 2015. Key objectives focus on improving the health of older people and those with long-term conditions and dementia.
The Mandate declares that mental health should be given equal priority to physical health, and commits the Government and NHSCB to support decentralisation and local decision-making. Its publication follows a period of consultation after the publication of a draft mandate, which was criticised for being too vague about its aims.
Robert Francis QC, chair of the Mid Staffordshire NHS Foundation Trust Public Inquiry, presents his final report to the Secretary of State for Health.
Originally due to report in October 2012, the Inquiry looked at how commissioning, regulatory and supervising bodies responded to the Mid Staffordshire NHS Foundation Trust’s problems between 2005 and 2009.
The final report, published on Wednesday 6 February 2013, addresses a range of issues of concern to NHS managers, clinical staff and patients, including: the recruitment, training and competency of staff; the regulation of care services; the science of quality measurement; the role of public voice and oversight; and the degree to which those working in the NHS feel empowered and engaged.
Set up in 2010 by the coalition Government, the Public Inquiry looked to build on a previous inquiry in 2008, also chaired by Robert Francis QC, which looked at individual cases of patient care.
Nuffield Trust Director of Policy Dr Judith Smith acted as an assessor to the Public Inquiry. Responding to the publication of the final report in February 2013, Dr Smith said: "We must not ignore the central implication of this report – namely, that within parts of the NHS dignity, care and compassion are routinely absent from the care of patients. The temptation may otherwise be to convince ourselves that the key lessons have already been learnt and improvements made."
In February 2014, the Nuffield Trust published a report exploring the impact of the Francis Report after one year. The research found that financial pressures and a complex regulatory environment are making it difficult for hospitals to create the kind of patient-centred culture recommended in the report.
And from April 2015, clearer entitlements and protection to ensure no-one will have to sell their home in their lifetime to pay for residential care.
In a Nuffield Trust statement in response to the announcement of the proposed reforms, Chief Economist Anita Charlesworth said:
"Whilst today’s announcement is not the solution to all the problems of the social care system, reforming funding in line with the Dilnot principles is an important and very welcome step in the right direction."
The 'new' NHS comes into being as responsibilities shift to bodies created by the 2012 Health and Social Care Act.
Primary care trusts (PCTs) are abolished. Their functions pass to NHS England (previously known as the NHS Commissioning Board) and the 211 clinical commissioning groups (CCGS) it has authorised.
CCGs which are only partially authorised are subject to special conditions from NHS England as they take on their new role. Some remain unauthorised, staying in ‘shadow’ form while NHS England takes on commissioning directly. CCGs will be supported by a number of commissioning support units (CSUs), which will provide a range of business functions designed to help CCGs improve services.
Strategic health authorities (SHAs) are also abolished. Health Education Englandtakes on SHAs’ responsibility for education, training and workforce development.
The NHS Trust Development Authoritytakes on responsibility for providing governance and accountability for NHS trusts and for delivering the foundation trust pipeline.
Four regional and 27 local branches of NHS England take on responsibility for the strategic oversight of provision and commissioning in their areas. Public health responsibilities are transferred to local authorities. Public Health England is established to improve the nation’s health and wellbeing and reduce inequalities.
New health and wellbeing boards are established. An independent consumer champion – Healthwatch England– is also created.
As the NHS reaches retirement age, political and clinical leaders call for a long term vision for the NHS.
To mark the 65th anniversary, the Nuffield Trust carried out a number of activities to reflect on the present state of the NHS and what it might look like in ten years’ time.
An agreement is made on the Pharmaceutical Price Regulation Scheme.
An agreement is established between the Department of Health and the Association of the British Pharmaceutical Industry (ABPI) was made in November 2013 on the Pharmaceutical Price Regulation Scheme.
This scheme would provide assurance on most of the branded medicine bills for the NHS, which would stay flat over the next two years and grow slowly after that. If NHS spending on branded medicines exceeds the allowed growth rate, then the pharmaceutical industry would make payments to the Department of Health.
7.3% UK spending on the NHS as a share of GDP
November 2013
The Government responds to the Francis Inquiry Report on the Mid Staffordshire NHS Foundation Trust Public Inquiry.
Following the Francis Inquiry final report in February 2013 the Government published their full response in November 2013. The full response focused strongly on new legislation and guidance to hospital trusts and their employees, planning to make the NHS more open, accountable and focused on safety and compassion.
7.3% UK spending on the NHS as a share of GDP
Image credit: Nuffield Trust
April 2014
Anniversary of the NHS reforms and Simon Stevens begins as Chief Executive of NHS England.
The 1 April 2014 marked the first anniversary of the implementation of the Coalition Government’s NHS reforms; including the introduction of clinical commissioning groups (CCGs). To mark this milestone the Nuffield Trust and The King’s Fund conducted a survey of GPs from six CCGs exploring member engagement and primary care development one year on. The anniversary also marked Simon Stevens becoming the new Chief Executive of NHS England.
The Coalition Government’s Care Bill receives its Royal Assent. The Bill looks to reform the law relating to adults and carers, to make provision for safeguarding adults from abuse or neglect; establishes Health Education England and the Health Research Authority; and makes provisions for care standards.
For the first time, the partner organisations that deliver and oversee health and care services including NHS England, Public Health England, Monitor, Health Education England, the Care Quality Commission and the NHS Trust Development Authority set out a shared vision for the future of the NHS in England. The Five Year Forward View outlines how the NHS needs to change over the next five years if it is to reduce health inequalities, improve the quality of care and meet an estimated £30 billion gap in funding by 2020/21.
Advised by the Nuffield Trust and other independent experts, the report outlines a number of options for how local health communities can create new ways of organising and delivering patient care. With no ‘one size fits all’ care model in mind, the report examines how groups of GPs may combine with nurses, other community health services, hospital specialists and mental health and social care to create integrated out-of-hospital care – so-called 'Multispecialty Community Providers'.
A further new option will be the integrated hospital and primary care provider – so-called 'Primary and Acute Care Systems', which would combine for the first time general practice and hospital services (in a similar way to the Accountable Care Organisations now developing in other countries).
7.25% UK spending on the NHS as a share of GDP
Image credit: Nuffield Trust
December 2014
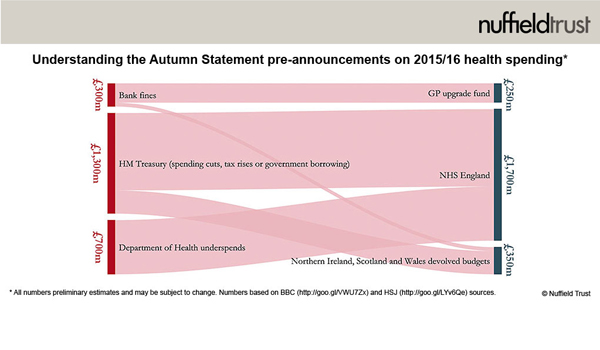
Autumn Statement injects £2 billion into the NHS budget for 2015/16.
“In many countries politicians are stepping back from detailed operational management of complex health services. But Labour’s proposals still feel somewhat top-down.”
Labour announce their Ten Year Plan for Health and Care.
The Ten Year Plan announced by Shadow Secretary for Health RT Hon Andy Burnham MP promised 36,000 new staff and the repeal of privatisation laws under a Labour government.
7.29% UK spending on the NHS as a share of GDP
“Local leaders in Manchester will find tension between the ‘N’ in NHS and local decision-making. Experience with the NHS in Wales illustrates how politicised this can get as responsibility for difficult decisions is transferred away from Westminster.”
Nigel Edwards, Chief Executive, Nuffield Trust, media releases
February 2015
Greater Manchester announces new devolved powers.
Greater Manchester announces plans to become the first English region to get full control of its health spending, as part of an extension of devolved powers.
7.29% UK spending on the NHS as a share of GDP
May 2015
The Conservative Party form a majority government
In an election result that confounded the pollsters and public alike, the Conservatives form a majority government, securing 331 seats in the House of Commons.
Conservative manifesto pledges for health include a focus on further implementing NHS England’s Five Year Forward View, seven-day access to a GP, 5,000 more GPs and a pledge of at least £8bn a year in additional funding for the NHS by 2020.
In the week following the election, David Cameron confirmed the first all-Conservative team of health ministers since 1997, with Jeremy Hunt continuing in his position as Health Secretary, whilst Alistair Burt replaces Norman Lamb as Minister of State.
7.29% UK spending on the NHS as a share of GDP
“£600m of NHS England’s 'extra' £8bn will be funded through cuts from public health.”
The Spending Review presented by Chancellor George Osborne announced a £3.8bn above inflation increase in funding for the NHS in England next year, as well as new measures to ease the pressures on local authorities with responsibilities for delivering social care. Public health was a casualty, losing £600 million.
7.29% UK spending on the NHS as a share of GDP
January 2016
Junior doctors vote overwhelmingly in favour of strike
After two years of abortive contract negotiations, in January and February 2016, junior doctors took strike action for the first time in forty years.
7.29% UK spending on the NHS as a share of GDP
“The NHS will feel very different, even in areas pursuing more limited models of devolution.”
Mark Dayan, Policy Analyst, Nuffield Trust
January 2016
The Cities & Local Government Devolution Bill is passed.
The Cities & Local Government Devolution Bill lays the foundation for a historic devolution of powers to local areas, with potentially momentous implications for the NHS. The Bill allows Secretaries of State to remove duties and powers from public bodies, including NHS trusts and commissioners, and transfer them to local councils or combined city authorities like Manchester.
As the Bill came into effect, the Nuffield Trust raised concerns about where accountability would lie in an increasingly devolved NHS with different commissioning and oversight arrangements across the country. We have called for an honest conversation about some of the uncertainties that remain.
7.26% UK spending on the NHS as a share of GDP
April 2016
NHS Improvement launches
At the beginning of the new financial year, Monitor, which regulates NHS foundation trusts, and the Trust Development Authority, which oversees other trusts, merged into one organisation. This single body, NHS Improvement, now has regulatory and oversight duties over all NHS providers under the governance of one Chief Executive - Jim Mackey.
7.26% UK spending on the NHS as a share of GDP
Image credit: GOV.uk
“Ideally, all the cash would be available for investment in new services and models of care. In reality, most of next year’s fund – £1.8bn of it – will be spent on bailing out NHS providers in deficit, leaving just £339m to fund 'transformation'.”
Draft Sustainability and Transformation Plans are submitted.
Sustainability and Transformation Plans (STPs) are local documents intended to spell out how NHS England’s ambitions for radical change in the health service over the next five years will actually happen across England.
There are 44 STP ‘footprint’ areas in total, each spanning multiple CCGs and trusts and convened by one local leader. In April 2016 each STP was required to submit their initial plans for their area, including a diagnosis of their major local challenges now and in the coming years and recommended actions to solve them.
A “Sustainability and Transformation Fund” worth £2.1 billion in its first year has been provided to support the activities of STPs, with release ultimately conditional on leaders being able to demonstrate that their local plans are effective. However, Nuffield Trust analysts voiced concerns that much of this funding would be absorbed by hospital deficits, leaving just £339 million to fund real transformation.
7.26% UK spending on the NHS as a share of GDP
May 2016
New contract agreed for junior doctors
An increasingly bitter dispute had seen saw more junior doctor strikes in March and April but a new contract was agreed between the BMA, NHS Employers and the Health Secretary on 18 May.
Initially rejected by junior doctors, and with more industrial action threatened but then abandoned, the contract eventually comes into force in October 2016.
7.3% UK spending on the NHS as a share of GDP
June 2016
The UK votes to leave the European Union
In a historic referendum result the UK voted by a narrow margin to leave the EU, leading to the resignation of David Cameron as Prime Minister.
While the long-term consequences of ‘Brexit’ for the public finances remain so far unclear, most analysts expect weaker growth for a time. This would have implications for NHS funding, along with the rest of the public sector.
Other critical areas include regulation – particularly the scrapping of the EU working time directive which controls the hours of NHS staff.
The health workforce too faces uncertainty. EU migrants make up a significant proportion of NHS staff – over 10 per cent of doctors and five per cent of nurses. Given the UK’s reliance on recruiting staff from overseas, the restriction of immigrants from Europe made possible by Brexit could exacerbate staffing issues in the health service.
Many academic institutions have also raised concerns about the loss of research funding from the EU on health and social care in the UK.
7.29% UK spending on the NHS as a share of GDP
“I worry what happens next. I fear that in order for hospitals to virtually eradicate their deficits as NHS Improvement and NHS England want, the next steps could be brutal service reductions and bed closures - which will shock an unprepared public.”
Nigel Edwards, Chief Executive, Nuffield Trust
July 2016
NHS leaders announce set of measures to regain control of NHS finances
National bodies NHS Improvement and NHS England announced a set of high profile interventions to ‘reset’ the NHS finances and tackle an increasing provider deficit of £2.45 billion.
The plans include a special measures regime for hospitals with the worst financial performance, and a series of controls resetting the total amount that provider trusts can spend. The new developments also mean hospitals will no longer be fined for missing key targets including the four hour A&E waiting time. Instead, hospitals will have to demonstrate that they have made agreed improvements in these areas in order to access part of the 2016 Sustainability Fund of £1.8 billion.
7.26% UK spending on the NHS as a share of GDP
“We do not yet have enough detail to know whether these plans can close the financial gap. Some look optimistic, but there are concerns about the time available, the scale of change and that many of the plans are based on experimental assumptions.”
Sustainability and Transformation Plans (STPs) published
The STPs set out shared proposals between local councils and NHS organisations to join up services within 44 localised ‘footprint’ areas and deal with the funding shortfalls up to 2020. STP leads were tasked with drawing up plans based on the needs of their local populations, covering a period of five years, to improve the quality and efficiency of services in their area. When inspecting some of the plans, many commentators – including our Chief Executive Nigel Edwards – noted that savings assumptions were ambitious within the timescale they had been given.
7.26% UK spending on the NHS as a share of GDP
March 2017
NHS England publishes Next steps on the Five Year Forward View.
June 2017
General Election 2017
The 2017 General Election was called early by Prime Minister Theresa May. The Conservative Party ultimately did not hold onto their majority in Parliament, and following the election had to rely on a confidence and supply arrangement with Northern Ireland’s Democratic Unionist Party.
For the first time in a British election social care was among the most prominent issues of the campaign. The Conservatives campaigned on a proposal to equalise the criteria for councils to pay for people in care homes and people receiving care in their own houses, and for more people to pay themselves by selling their homes when they died. The policy was widely criticised, and amended during the campaign. The incoming Government pledges a Green Paper on social care as one of its priorities.
7.18% UK spending on the NHS as a share of GDP
June 2018
Funding settlement announced for the NHS ahead of 70th anniversary
Theresa May announced that the NHS will receive an average yearly real terms spending increase of 3.4% for the next five years, marking a step change from rises of around 1% over the previous ten years of austerity, yet still below the 4% experts recommended in order to meet patient need in the future.
The funding came alongside the announcement of a new 10 year plan for the NHS, which would also “tackle waste and improve services”.
The announcement is regarded as a “big step forward”, however, Nuffield Trust CEO Nigel Edwards warns that whilst this offers much needed respite for the NHS, its growing workforce issues and deficits will make it very difficult to achieve The Prime Minister’s ambition to create a world-class health service with spending increases of less than the historic average.
7.1% UK spending on the NHS as a share of GDP
New GP contract heralds major change in the primary care workforce
January 2019
A new contract for general practice is agreed between the BMA and NHS England
A new contract is agreed for general practice opening the way for GPs to deliver a much wider range of services, to build larger primary care networks and to develop wider multi-disciplinary teams involving pharmacists and physiotherapists as first contact providers.
Nigel Edwards describes the move as a radical step that should help relieve some of the pressures GPs face. “It is likely to lead to a historic move away from GPs as freestanding small businesses. We’re pleased this is being done through the carrot, not the stick.”
For more information on the historic changes made to the GP contract, read this short explainer originally produced for the WHO/EU European Observatory on Health Systems and Policies.
7.1% UK spending on the NHS as a share of GDP
January 2019
NHS England publishes the Long Term Plan.
The document aims to set the direction of the health service across the ten years to 2028. The plan includes ambitious goals to reduce the number of avoidable deaths from cancer, heart disease, and stroke, and to put in place crisis care teams that respond within two hours. It calls for GPs across England to join networks and to offer all patients online consultations. Local health and social care services are to come together as “Integrated Care Systems” which combine commissioners and NHS trusts. The plan also sets out plans for legislative change to pool local powers, loosen competition requirements, and make it easier to combine the activities of NHS England and NHS Improvement.
For more information on the detail and context of the Long Term Plan, read this short explainer originally produced for the WHO/EU European Observatory on Health Systems and Policies.
7.10% UK spending on the NHS as a share of GDP
2020s
January 2020
The UK officially leaves the EU
Following the Brexit vote of June 2016, the United Kingdom officially leaves the European Union on 31 January 2020, although it remains a de facto member and beneficiary of its constituent structures until the end of the agreed transition period on 31 December 2020.
9.9% UK spending on the NHS as a share of GDP
Image credit: Wikimedia
February 2020
The emergence of Covid-19
A new coronavirus causing a condition called Covid-19 is declared a global pandemic by WHO in March 2020. The virus was first identified in December 2019 in Wuhan, China, and the first death in the UK is recorded on 28 February 2020, with Europe soon becoming the epicentre of the outbreak. On 23 March, the UK government implements a far-reaching lockdown which bars people from leaving their houses for any reason except food, medicine, daily exercise, and helping people with health needs. Schools, universities, and most shops are closed, and the state takes over paying many workers and self-employed people unable to work.
NHS England’s Chief Executive Sir Simon Stevens declares Covid-19 the greatest challenge the health service has ever faced. Elective operations are cancelled, student and retired clinicians are drafted in, and new hospital sites are opened to respond to the pandemic.
It soon emerges that UK Prime Minister Boris Johnson has contracted the virus, and spends three days in hospital intensive care in early April due to its effects.
Image credit: Wikimedia
December 2020
Vaccine development and further lockdown
The MHRA grants an emergency use authorisation on 2 December for a Covid-19 vaccine, by Pfizer-Biontech, and the UK is the first Western country to approve a vaccine. The NHS administered the first vaccine, in Coventry, on December 8. With other vaccines to combat the virus soon to follow, namely from Oxford AstraZeneca and Moderna, the NHS begins a significant programme to deliver these to UK citizens. The UK initially achieves rapid coverage of first doses relative to other countries, at the expense of delivering second doses at the recommended time.
Despite a fall in case and death numbers during the summer of 2020, numbers again rise as autumn approaches. Lighter forms of lockdown in England in late 2020 fail to achieve sustained reductions in cases, and the Alpha variant of Covid-19, first identified in Kent, causes a surge in cases and deaths in early 2021. A second major national lockdown is imposed from January to March.
9.9%% UK spending on the NHS as a share of GDP
Image credit: bbc.co.uk
November 2021
NHS waiting times hit new levels
Deaths due to Covid-19 reach 150,000 in the United Kingdom, but with more than 50 million UK adults and adolescents vaccinated against Covid-19, death numbers do fall significantly as the year progresses, despite case numbers staying high. A new Covid-19 variant – Omicron – is first identified in South Africa, and by the end of November is the cause of cases in the UK. In the same month, the NHS waiting list in England passes 6 million – equivalent to more than a tenth of the population.
9.9%% UK spending on the NHS as a share of GDP
Image credit: The Guardian
May 2022
Health and Care Act 2022
The Health and Care Act 2022 passes through Parliament, setting in place a restructure of the English NHS around “Integrated Care Systems” and strengthening the control of the Secretary of State for Health.
9.9% UK spending on the NHS as a share of GDP
About
With thanks to Geoffrey Rivett, contemporary health historian and author of the website www.nhshistory.net, for his help in editing and reviewing the timeline content.